

Pancreatic β-cell proliferation in obesity
- PMID: 24829474
- PMCID: PMC4013180
- DOI: 10.3945/an.113.005488
Pancreatic β-cell proliferation in obesity
Abstract
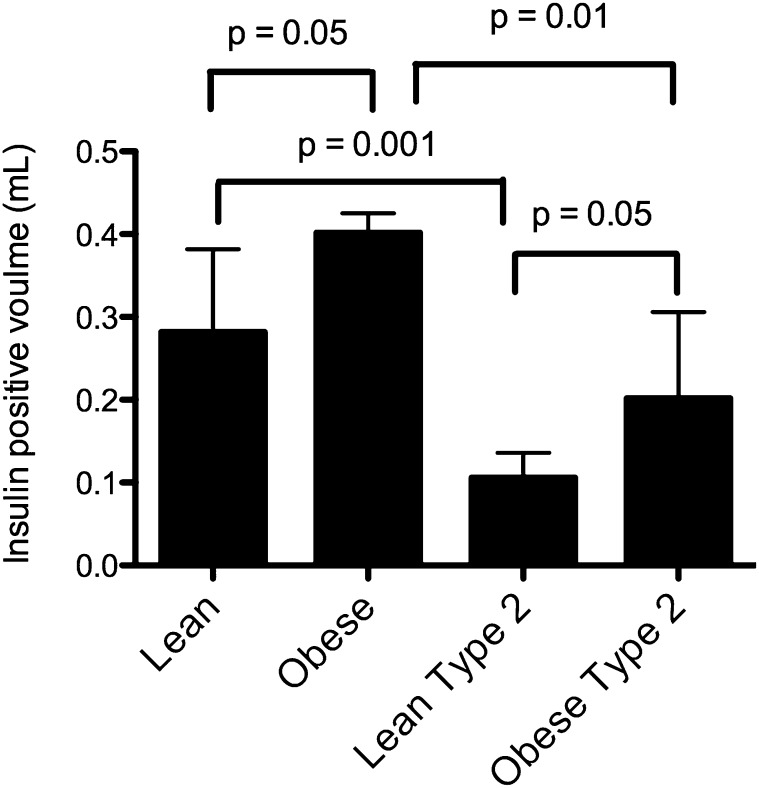
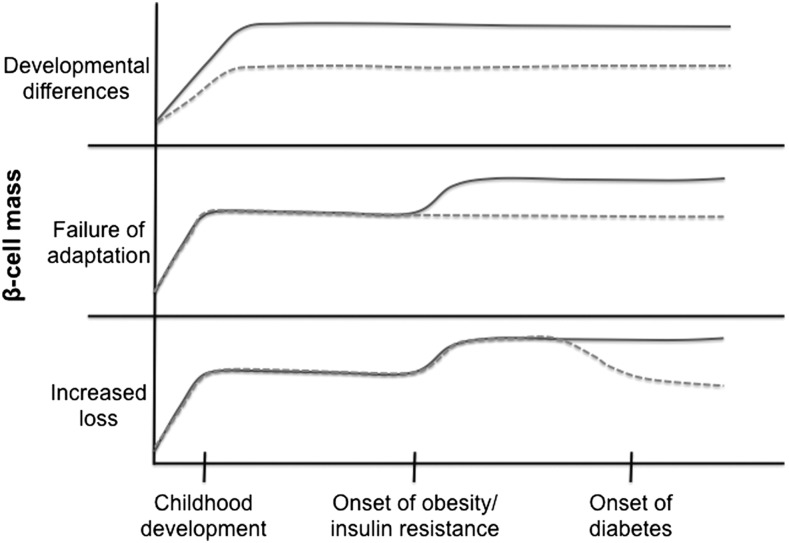
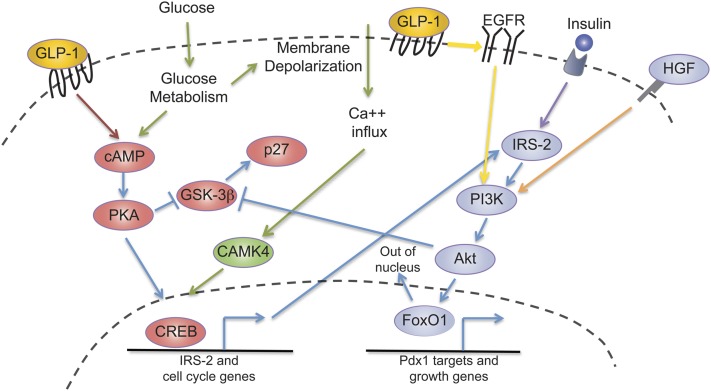
Because obesity rates have increased dramatically over the past 3 decades, type 2 diabetes has become increasingly prevalent as well. Type 2 diabetes is associated with decreased pancreatic β-cell mass and function, resulting in inadequate insulin production. Conversely, in nondiabetic obesity, an expansion in β-cell mass occurs to provide sufficient insulin and to prevent hyperglycemia. This expansion is at least in part due to β-cell proliferation. This review focuses on the mechanisms regulating obesity-induced β-cell proliferation in humans and mice. Many factors have potential roles in the regulation of obesity-driven β-cell proliferation, including nutrients, insulin, incretins, hepatocyte growth factor, and recently identified liver-derived secreted factors. Much is still unknown about the regulation of β-cell replication, especially in humans. The extracellular signals that activate proliferative pathways in obesity, the relative importance of each of these pathways, and the extent of cross-talk between these pathways are important areas of future study.
© 2014 American Society for Nutrition.
Conflict of interest statement
Author disclosures: A. K. Linnemann, M. Baan, and D. B. Davis, no conflicts of interest.
Figures
References
-
- Ogden CL, Carroll ME, Kit BK, Flegal KM. Prevalence of obesity in the United States, 2009#x20132010. NCHS Data Brief. 2012;82:1#x20138. - PubMed
-
- Centers for Disease Control and Prevention. National diabetes fact sheet: national estimates and general information on diabetes and prediabetes in the United States, 2011. U.S. Department of Health and Human Services; 2011.
-
- Ritzel RA, Butler AE, Rizza RA, Veldhuis JD, Butler PC. Relationship between beta-cell mass and fasting blood glucose concentration in humans. Diabetes Care. 2006;29:717–8 - PubMed
-
- Klöppel G, Löhr M, Habich K, Oberholzer M, Heitz PU. Islet pathology and the pathogenesis of type 1 and type 2 diabetes mellitus revisited. Surv Synth Pathol Res. 1985;4:110–25 - PubMed
-
- Butler AE, Janson J, Bonner-Weir S, Ritzel R, Rizza RA, Butler PC. Beta-cell deficit and increased beta-cell apoptosis in humans with type 2 diabetes. Diabetes. 2003;52:102–10 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
