

Neuroendocrine carcinoma of the stomach: A case report
- PMID: 24829627
- PMCID: PMC4013715
- DOI: 10.4240/wjgs.v6.i4.77
Neuroendocrine carcinoma of the stomach: A case report
Abstract
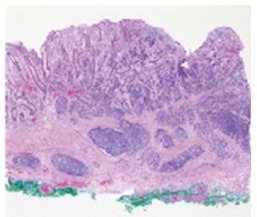
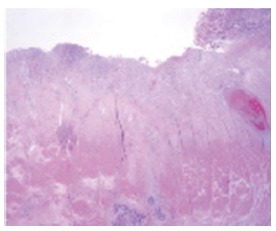
Neuroendocrine carcinoma (NEC) is a rare tumor, comprising < 1% of stomach cancers. A 55-year-old woman was referred to our hospital with biopsy-proven gastric cancer. A shallow ulcerative lesion was detected in the lesser curvature of the lower body. It was suspected to be early gastric cancer IIA + IIC type. Thus, endoscopic submucosal dissection was performed. She was subsequently diagnosed with NEC, which is aggressive and carries a poor prognosis. We conducted a radical resection and a laparoscopic-assisted distal gastrectomy. The tumor had infiltrated the subserosal layer and 6/42 lymph nodes were involved. The mitotic index was 16/10 high power fields and the Ki-67 labeling index was 26%-50%. The final diagnosis of NEC was made according to the World Health Organization 2010 criteria. She was suspected of having jumping metastasis to the proximal margin. The patient was treated with an oral anticancer drug (5-flurouracil based drug) for 2 years. The patient has been followed up for 3 years without recurrence.
Keywords: Gastrectomy; Ki-67; Mitosis; Neuroendocrine carcinoma; Prognosis.
Figures

References
-
- Rindi G, Bordi C, Rappel S, La Rosa S, Stolte M, Solcia E. Gastric carcinoids and neuroendocrine carcinomas: pathogenesis, pathology, and behavior. World J Surg. 1996;20:168–172. - PubMed
-
- Rindi G. Clinicopathologic aspects of gastric neuroendocrine tumors. Am J Surg Pathol. 1995;19 Suppl 1:S20–S29. - PubMed
-
- The International Agency for Research on Cancer. WHO Classification of Tumors of the Digestive System. 4th edition. Bosman FT, Carneiro F, Hruban RH, Theise ND, editor. Lyon: International Agency of Research of Cancer; 2010. pp. 53–57.
-
- Modlin IM, Oberg K, Chung DC, Jensen RT, de Herder WW, Thakker RV, Caplin M, Delle Fave G, Kaltsas GA, Krenning EP, et al. Gastroenteropancreatic neuroendocrine tumours. Lancet Oncol. 2008;9:61–72. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
