

Triple Diuretics and Aquaretic Strategy for Acute Decompensated Heart Failure due to Volume Overload
- PMID: 24829808
- PMCID: PMC4008352
- DOI: 10.1155/2013/750794
Triple Diuretics and Aquaretic Strategy for Acute Decompensated Heart Failure due to Volume Overload
Abstract
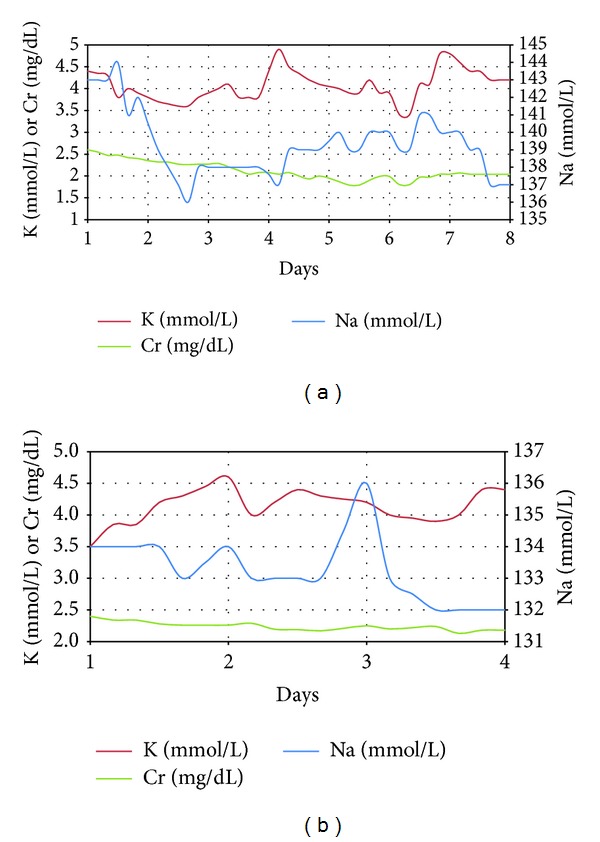
Diuretics, including furosemide, metolazone, and spironolactone, have historically been the mainstay of therapy for acute decompensated heart failure patients. The addition of an aquaretic-like vasopressin antagonist may enhance diuresis further. However, clinical experience with this quadruple combination is lacking in the acute setting. We present two hospitalized patients with acute decompensated heart failure due to massive fluid overload treated with a combination strategy of triple diuretics in conjunction with the aquaretic tolvaptan. The first patient lost 72.1 lbs. (32.7 kg) with an average urine output of 3.5 to 7.5 L/day over eight days on combined therapy with furosemide, metolazone, spironolactone, and tolvaptan. The second patient similarly achieved a weight loss of 28.2 lbs. (12.8 kg) over 4 days on the same treatment. Both patients maintained stable serum sodium, potassium, and creatinine over this period and remained out of the hospital for more than 30 days. Thus, patients hospitalized with acute decompensated heart failure due to volume overload can achieve euvolemia rapidly and without electrolytes disturbances using this regimen, while being under the close supervision of a team of cardiologists and nephrologists. Additionally, this therapy can potentially decrease the need for ultrafiltration and the length of hospital stay.
Figures
References
-
- Sarraf M, Masoumi A, Schrier RW. Cardiorenal syndrome in acute decompensated heart failure. Clinical Journal of the American Society of Nephrology. 2009;4(12):2013–2026. - PubMed
-
- Krämer B, Schweda F, Riegger G. Diuretic treatment and diuretic resistance in heart failure. American Journal of Medicine. 1999;106(1):90–96. - PubMed
-
- Paul S. Balancing diuretic therapy in heart failure: Loop diuretics, thiazides, and aldosterone antagonists. Congestive Heart Failure. 2002;8(6):307–312. - PubMed
-
- Masatsugu H. Tolvaptan for heart failure patients with volume overload. Cardiovascular Drugs and Therapy. 2011;25(1, supplement 1):S1–S4. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
