

Deregulation of microcephalin and ASPM expression are correlated with epithelial ovarian cancer progression
- PMID: 24830737
- PMCID: PMC4022499
- DOI: 10.1371/journal.pone.0097059
Deregulation of microcephalin and ASPM expression are correlated with epithelial ovarian cancer progression
Abstract
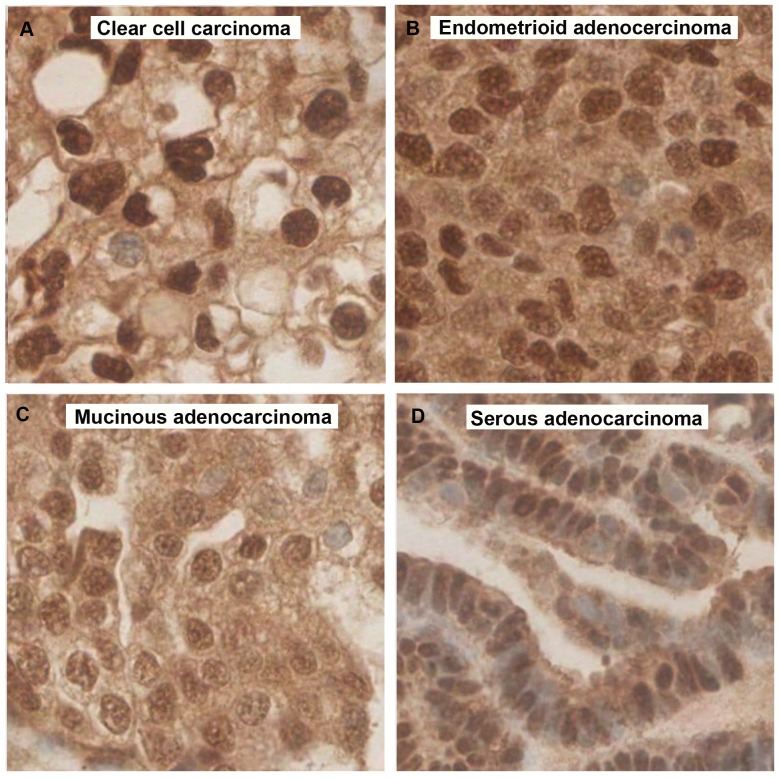
Mutations in the MCPH1 (Microcephalin) and ASPM (abnormal spindle-like microcephaly associated) genes cause primary microcephaly. Both are centrosomal associated proteins involved in mitosis. Microcephalin plays an important role in DNA damage response and ASPM is required for correct division of proliferative neuro-epithelial cells of the developing brain. Reduced MCPH1 mRNA expression and ASPM mRNA over-expression have been implicated in the development of human carcinomas. Epithelial ovarian cancer (EOC) is characterised by highly aneuploid tumours. Previously we have reported low Microcephalin and high ASPM protein levels and associations with clinico-pathological parameters in malignant cells from ascitic fluids. To confirm these previous findings on a larger scale Microcephalin and ASPM expression levels and localisations were evaluated by immunohistochemistry in two cohorts; a training set of 25 samples and a validation set of 322 EOC tissue samples. Results were correlated to the associated histopathological data. In normal ovarian tissues the Microcephalin nuclear staining pattern was consistently strong. In the cancer tissues, we identified low nuclear Microcephalin expression in high grade and advanced stage tumours (p<0.0001 and p = 0.0438 respectively). ASPM had moderate to high nuclear and low to moderate cytoplasmic expression in normal tissue. Cytoplasmic ASPM expression decreased with tumour grade and stage in the serous subtype of EOC (p = 0.023 and p = 0.011 respectively). Cytoplasmic ASPM increased with tumour stage in the endometrioid subtype (p = 0.023). Increasing tumour invasiveness (T3) and lymph node involvement (N1) also correlated with a decrease in cytoplasmic ASPM in EOC (p = 0.02 and p = 0.04 respectively). We have validated previous findings of deregulated expression of Microcephalin and ASPM in EOC by confirming associations for low nuclear Microcephalin levels and high cytoplasmic ASPM levels in a larger scale tumour tissue study. Microcephalin and ASPM may prove useful biomarkers in EOC.
Conflict of interest statement
Figures






References
-
- Ferlay J, Shin HR, Bray F, Forman D, Mathers C, et al.. GLOBOCAN 2008 v1.2, Cancer Incidence and Mortality Worldwide.
-
- IARC Cancer base No. 10 [Internet] Lyon, France: International Agency for Research on Cancer, 2010. Available: http://globocan.iarc.fr.
-
- Auersperg N, Wong AS, Choi KC, Kang SK, Leung PC (2001) Ovarian surface epithelium: biology, endocrinology and pathology. Endocr Rev 22(2): 255–88. - PubMed
-
- Despierre E, Lambrechts D, Neven P, Amant F, Lambrechts S, et al. (2010) The molecular genetic basis of ovarian cancer and its roadmap towards a better treatment. Gynecol Oncol 117(2): 358–65. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
