

Development and validation of risk models to predict outcomes following in-hospital cardiac arrest attended by a hospital-based resuscitation team
- PMID: 24830872
- PMCID: PMC4111919
- DOI: 10.1016/j.resuscitation.2014.05.004
Development and validation of risk models to predict outcomes following in-hospital cardiac arrest attended by a hospital-based resuscitation team
Abstract
Aim: The National Cardiac Arrest Audit (NCAA) is the UK national clinical audit for in-hospital cardiac arrest. To make fair comparisons among health care providers, clinical indicators require case mix adjustment using a validated risk model. The aim of this study was to develop and validate risk models to predict outcomes following in-hospital cardiac arrest attended by a hospital-based resuscitation team in UK hospitals.
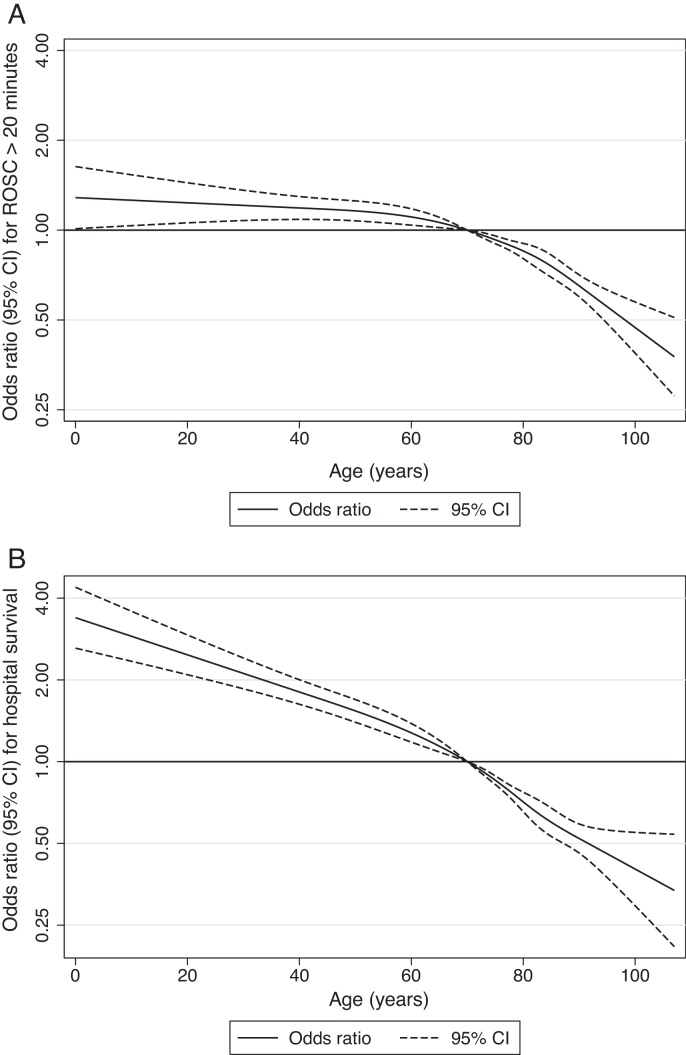
Methods: Risk models for two outcomes-return of spontaneous circulation (ROSC) for greater than 20min and survival to hospital discharge-were developed and validated using data for in-hospital cardiac arrests between April 2011 and March 2013. For each outcome, a full model was fitted and then simplified by testing for non-linearity, combining categories and stepwise reduction. Finally, interactions between predictors were considered. Models were assessed for discrimination, calibration and accuracy.
Results: 22,479 in-hospital cardiac arrests in 143 hospitals were included (14,688 development, 7791 validation). The final risk model for ROSC>20min included: age (non-linear), sex, prior length of stay in hospital, reason for attendance, location of arrest, presenting rhythm, and interactions between presenting rhythm and location of arrest. The model for hospital survival included the same predictors, excluding sex. Both models had acceptable performance across the range of measures, although discrimination for hospital mortality exceeded that for ROSC>20min (c index 0.81 versus 0.72).
Conclusions: Validated risk models for ROSC>20min and hospital survival following in-hospital cardiac arrest have been developed. These models will strengthen comparative reporting in NCAA and support local quality improvement.
Keywords: Cardiopulmonary resuscitation; Heart arrest; Hospital mortality; Models; Risk adjustment; Statistical.
Copyright © 2014 The Authors. Published by Elsevier Ireland Ltd.. All rights reserved.
Figures

Similar articles
-
Risk-adjusted survival for adults following in-hospital cardiac arrest by day of week and time of day: observational cohort study.BMJ Qual Saf. 2016 Nov;25(11):832-841. doi: 10.1136/bmjqs-2015-004223. Epub 2015 Dec 11. BMJ Qual Saf. 2016. PMID: 26658774 Free PMC article.
-
Ensuring comparisons of health-care providers are fair: development and validation of risk prediction models for critically ill patients.Southampton (UK): NIHR Journals Library; 2015 Oct. Southampton (UK): NIHR Journals Library; 2015 Oct. PMID: 26491757 Free Books & Documents. Review.
-
Risk-Standardizing Rates of Return of Spontaneous Circulation for In-Hospital Cardiac Arrest to Facilitate Hospital Comparisons.J Am Heart Assoc. 2020 Apr 7;9(7):e014837. doi: 10.1161/JAHA.119.014837. Epub 2020 Mar 21. J Am Heart Assoc. 2020. PMID: 32200716 Free PMC article.
-
The landscape of paediatric in-hospital cardiac arrest in the United Kingdom National Cardiac Arrest Audit.Resuscitation. 2020 Oct;155:165-171. doi: 10.1016/j.resuscitation.2020.07.026. Epub 2020 Aug 6. Resuscitation. 2020. PMID: 32768496
-
Improving risk prediction model quality in the critically ill: data linkage study [Internet].Southampton (UK): National Institute for Health and Care Research; 2022 Dec. Southampton (UK): National Institute for Health and Care Research; 2022 Dec. PMID: 36542744 Free Books & Documents. Review.
Cited by
-
In-Hospital Cardiac Arrest: A Review.JAMA. 2019 Mar 26;321(12):1200-1210. doi: 10.1001/jama.2019.1696. JAMA. 2019. PMID: 30912843 Free PMC article. Review.
-
Prediction Models for Return of Spontaneous Circulation in Patients with Cardiac Arrest: A Systematic Review and Critical Appraisal.Emerg Med Int. 2023 Nov 21;2023:6780941. doi: 10.1155/2023/6780941. eCollection 2023. Emerg Med Int. 2023. PMID: 38035124 Free PMC article. Review.
-
Risk prediction models for out-of-hospital cardiac arrest outcomes in England.Eur Heart J Qual Care Clin Outcomes. 2021 Mar 15;7(2):198-207. doi: 10.1093/ehjqcco/qcaa019. Eur Heart J Qual Care Clin Outcomes. 2021. PMID: 32154865 Free PMC article.
-
Clinical Predictive Models of Sudden Cardiac Arrest: A Survey of the Current Science and Analysis of Model Performances.J Am Heart Assoc. 2020 Aug 18;9(16):e017625. doi: 10.1161/JAHA.119.017625. Epub 2020 Aug 13. J Am Heart Assoc. 2020. PMID: 32787675 Free PMC article.
-
Prognostic models for outcome prediction following in-hospital cardiac arrest using pre-arrest factors: a systematic review, meta-analysis and critical appraisal.Crit Care. 2023 Jan 20;27(1):32. doi: 10.1186/s13054-023-04306-y. Crit Care. 2023. PMID: 36670450 Free PMC article.
References
-
- Black N. Assessing the quality of hospitals. BMJ. 2010;340:c2066. - PubMed
-
- Krumholz H.M., Brindis R.G., Brush J.E. Standards for statistical models used for public reporting of health outcomes. Circulation. 2006;113:456–462. - PubMed
-
- Moons K.G.M., Royston P., Vergouwe Y., Grobbee D.E., Altman D.G. Prognosis and prognostic research: what, why, and how? BMJ. 2009;338:b375. - PubMed
-
- Peberdy M.A., Kaye W., Ornato J.P. Cardiopulmonary resuscitation of adults in the hospital: a report of 14720 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation. 2003;58:297–308. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
