

Baseline subclinical atherosclerosis burden and distribution are associated with frequency and mode of future coronary revascularization: multi-ethnic study of atherosclerosis
- PMID: 24831208
- PMCID: PMC4024837
- DOI: 10.1016/j.jcmg.2014.03.005
Baseline subclinical atherosclerosis burden and distribution are associated with frequency and mode of future coronary revascularization: multi-ethnic study of atherosclerosis
Abstract
Objectives: The aim of this study was to evaluate the impact of coronary artery calcium (CAC) burden and regional distribution on the need for and type of future coronary revascularization-percutaneous versus surgical (coronary artery bypass graft [CABG])-among asymptomatic subjects.
Background: The need for coronary revascularization and the chosen mode of revascularization are thought to be functions of disease burden and anatomic distribution. The association between the baseline burden and regional distribution of CAC and the risk and type of future coronary revascularization remains unknown.
Methods: A total of 6,540 participants in the MESA (Multi-Ethnic Study of Atherosclerosis) (subjects aged 45 to 84 years, free of known baseline cardiovascular disease) with vessel-specific CAC measurements were followed for a median of 8.5 years (interquartile range: 7.7 to 8.6 years). Annualized rates and multivariate-adjusted hazard ratios for revascularization and revascularization type were analyzed according to CAC score category, number of vessels with CAC (0 to 4, including the left main coronary artery), and involvement of individual coronary arteries.
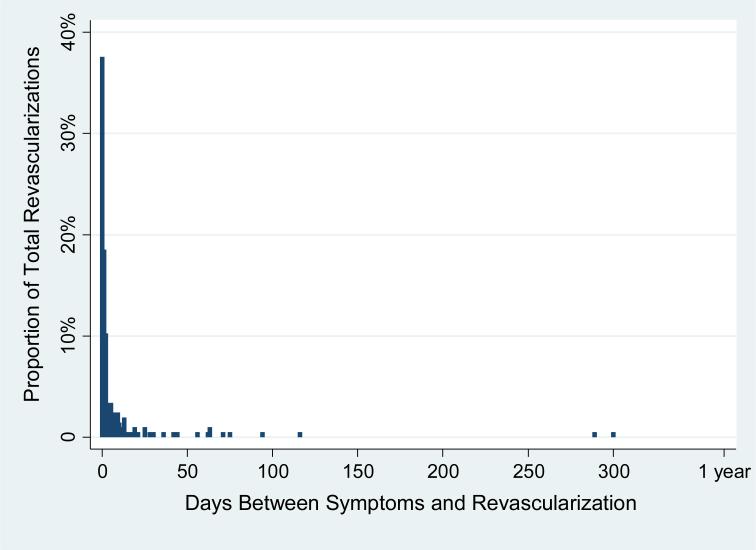
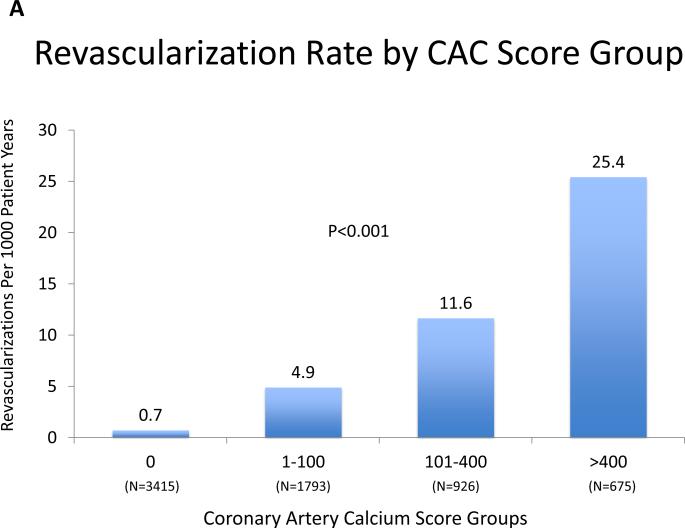
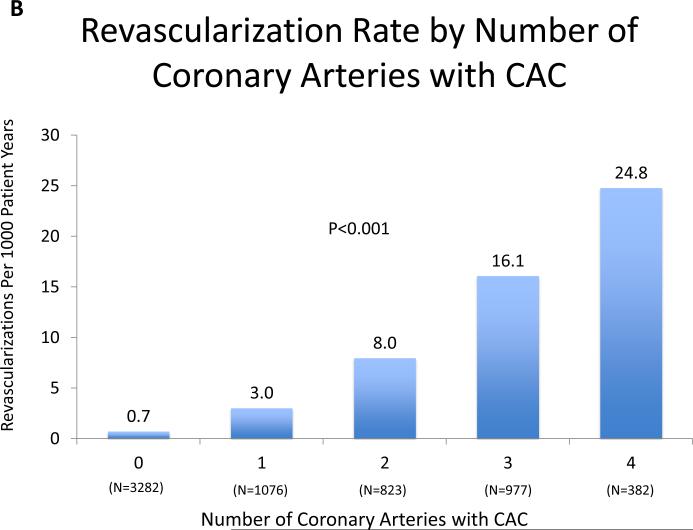
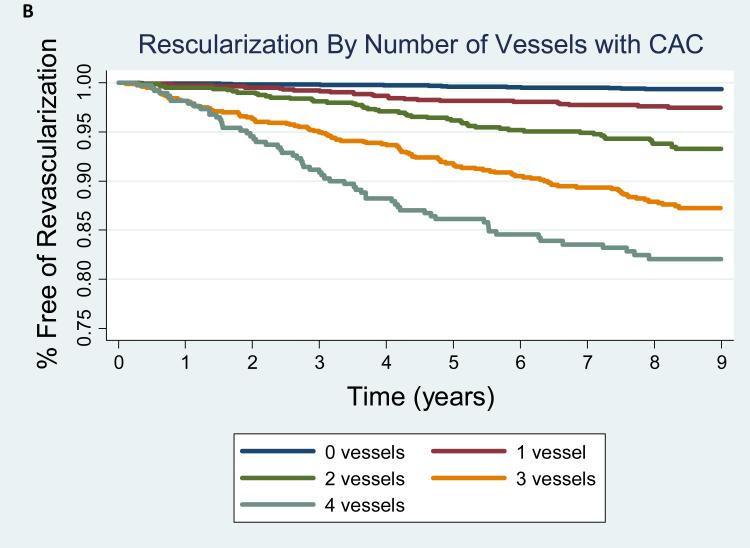
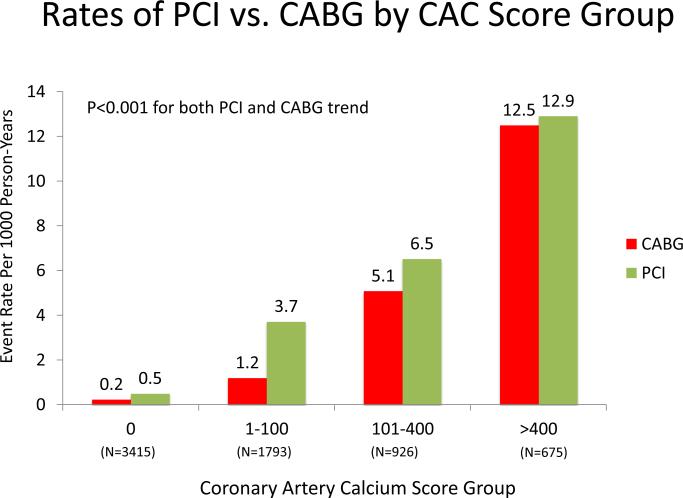
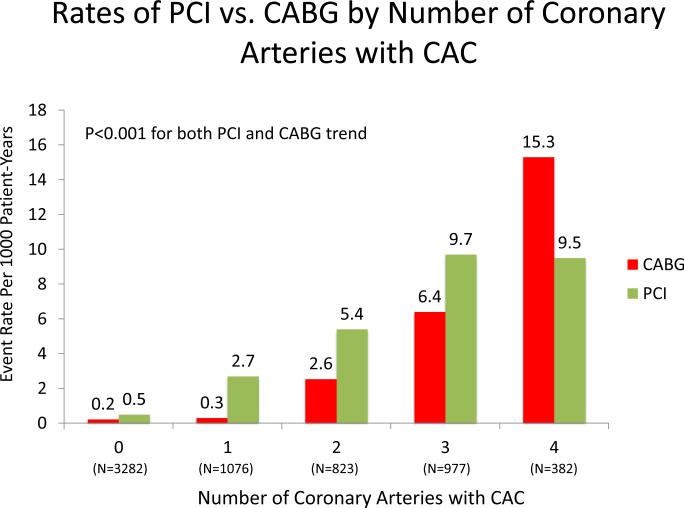
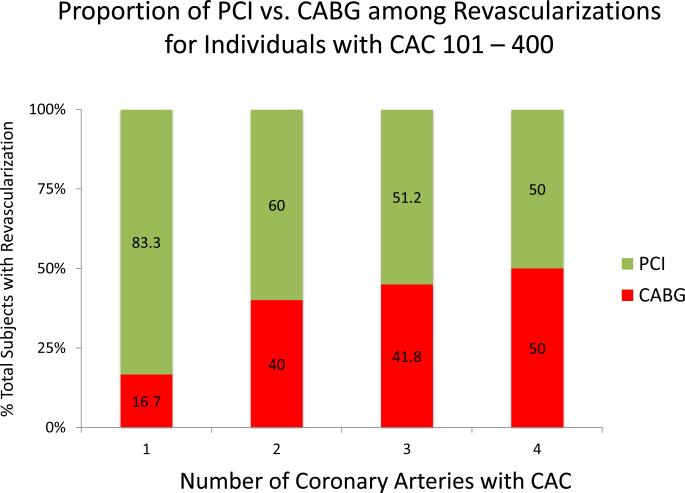
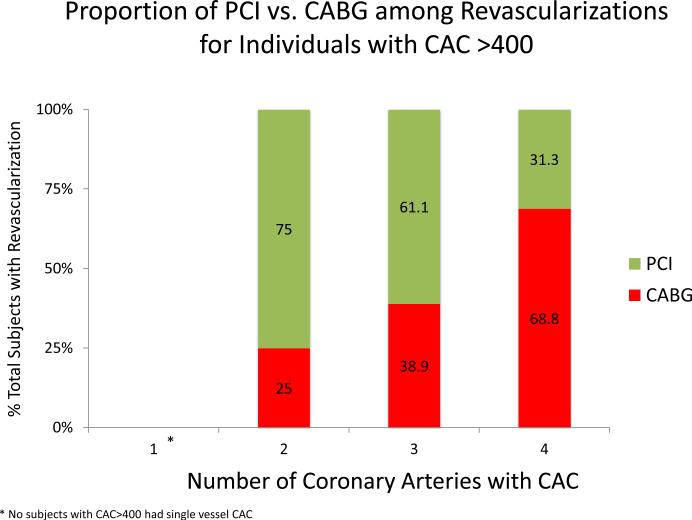
Results: A total of 265 revascularizations (4.2%) occurred during follow-up, and 206 (78% of the total) were preceded by adjudicated symptoms. Revascularization was uncommon when CAC score was 0.0 (0.6%), with a graded increase over both rising CAC burden and increasingly diffuse CAC distribution. The revascularization rates per 1,000 person-years for CAC scores of 1 to 100, 101 to 400, and >400 were 4.9, 11.7, and 25.4, respectively; for 1, 2, 3, and 4 vessels with CAC, the rates were 3.0, 8.0, 16.1, and 24.8, respectively. In multivariate models adjusting for CAC score, the number of vessels with CAC remained predictive of revascularization and mode of revascularization. Independent predictors of CABG versus percutaneous coronary intervention included 3- or 4-vessel CAC, higher CAC burden, and involvement of the left main coronary artery. Risk for CABG was extremely low with <3-vessel baseline CAC. Results were similar when considering only symptom-driven revascularizations.
Conclusions: In this multiethnic cohort of asymptomatic subjects, baseline CAC was highly predictive of future coronary revascularization procedures, with measures of CAC burden and distribution each independently predicting need for percutaneous coronary intervention versus CABG over an 8.5-year follow-up.
Keywords: cardiac CT; coronary artery calcium; coronary artery disease; revascularization.
Copyright © 2014 American College of Cardiology Foundation. Published by Elsevier Inc. All rights reserved.
Figures


Comment in
-
Coronary artery calcium score, distribution, and future revascularization.JACC Cardiovasc Imaging. 2014 May;7(5):487-9. doi: 10.1016/j.jcmg.2014.03.008. JACC Cardiovasc Imaging. 2014. PMID: 24831209 No abstract available.
References
-
- Detrano R, Guerci AD, Carr JJ, Bild DE, Burke G, Folsom AR, et al. Coronary calcium as a predictor of coronary events in four racial or ethnic groups. N Engl J Med. 2008;358(13):1336–45. - PubMed
-
- Greenland P, LaBree L, Azen SP, Doherty TM, Detrano RC. Coronary artery calcium score combined with Framingham score for risk prediction in asymptomatic individuals. JAMA. 2004;291(2):210–5. - PubMed
-
- Arad Y, Goodman KJ, Roth M, Newstein D, Guerci AD. Coronary calcification, coronary disease risk factors, C-reactive protein, and atherosclerotic cardiovascular disease events: the St. Francis Heart Study. J Am Coll Cardiol. 2005;46(1):158–65. - PubMed
-
- LaMonte MJ, FitzGerald SJ, Church TS, Barlow CE, Radford NB, Levine BD, et al. Coronary artery calcium score and coronary heart disease events in a large cohort of asymptomatic men and women. Am J Epidemiol. 2005;162(5):421–9. - PubMed
-
- Sarwar A, Shaw LJ, Shapiro MD, Blankstein R, Hoffmann U, Hoffman U, et al. Diagnostic and prognostic value of absence of coronary artery calcification. JACC Cardiovasc Imaging. 2009;2(6):675–88. - PubMed
Publication types
MeSH terms
Grants and funding
- N01-HC-95162/HC/NHLBI NIH HHS/United States
- L30 HL110027/HL/NHLBI NIH HHS/United States
- N01 HC095169/HL/NHLBI NIH HHS/United States
- N01-HC-95159/HC/NHLBI NIH HHS/United States
- N01-HC-95165/HC/NHLBI NIH HHS/United States
- N01 HC095159/HL/NHLBI NIH HHS/United States
- T32 HL007227/HL/NHLBI NIH HHS/United States
- N01-HC-95160/HC/NHLBI NIH HHS/United States
- N01-HC-95166/HC/NHLBI NIH HHS/United States
- N01-HC-95167/HC/NHLBI NIH HHS/United States
- N01-HC-95163/HC/NHLBI NIH HHS/United States
- N01-HC-95168/HC/NHLBI NIH HHS/United States
- N01-HC-95169/HC/NHLBI NIH HHS/United States
- N01-HC-95164/HC/NHLBI NIH HHS/United States
- N01-HC-95161/HC/NHLBI NIH HHS/United States
- T32-HL-7227-36/HL/NHLBI NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical