

HIV-infected individuals with low CD4/CD8 ratio despite effective antiretroviral therapy exhibit altered T cell subsets, heightened CD8+ T cell activation, and increased risk of non-AIDS morbidity and mortality
- PMID: 24831517
- PMCID: PMC4022662
- DOI: 10.1371/journal.ppat.1004078
HIV-infected individuals with low CD4/CD8 ratio despite effective antiretroviral therapy exhibit altered T cell subsets, heightened CD8+ T cell activation, and increased risk of non-AIDS morbidity and mortality
Abstract
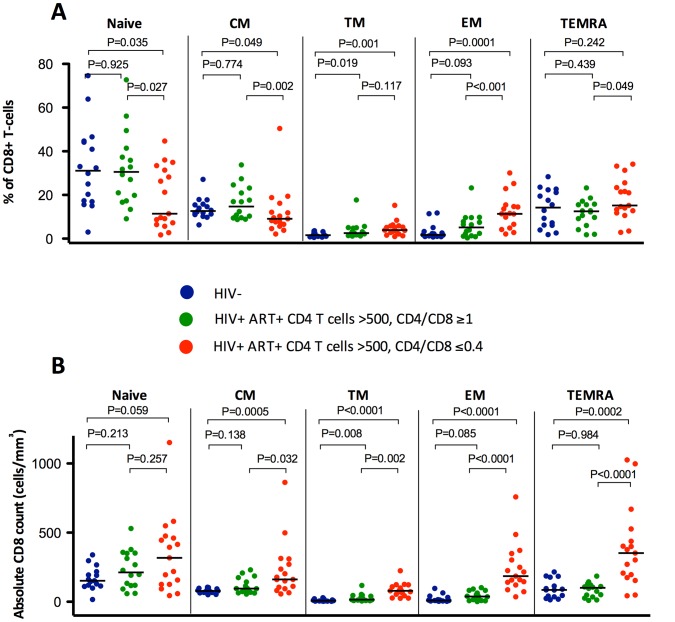
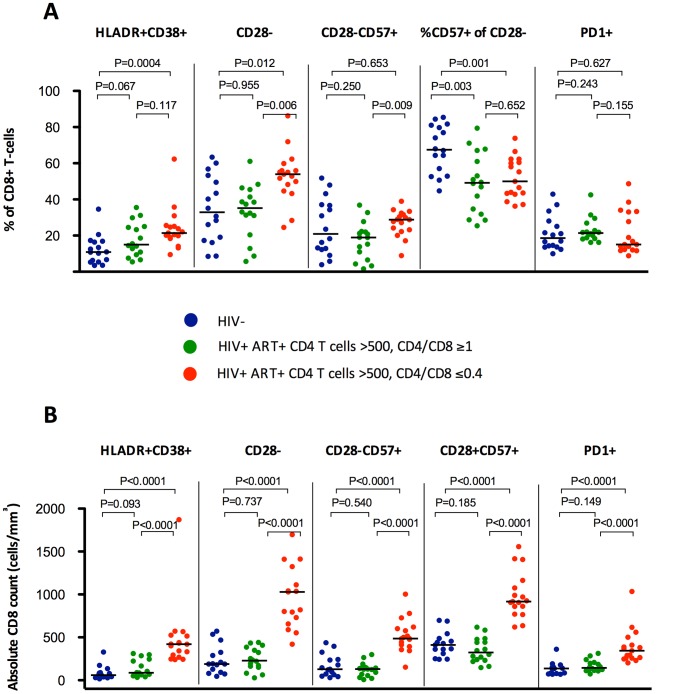
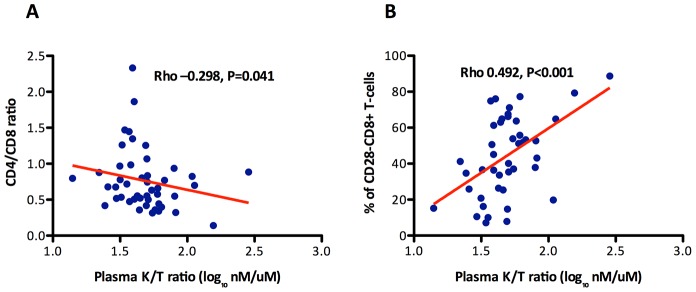
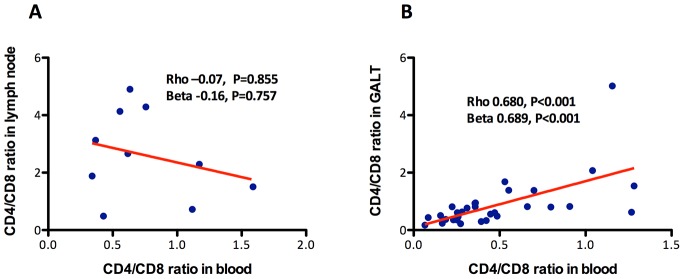
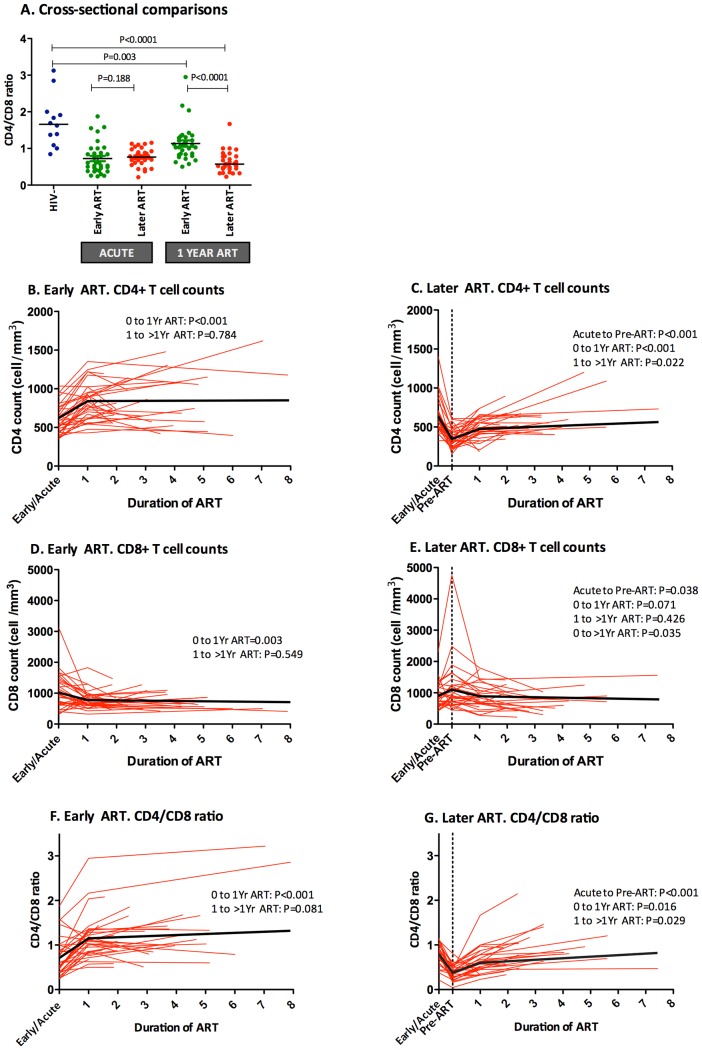
A low CD4/CD8 ratio in elderly HIV-uninfected adults is associated with increased morbidity and mortality. A subset of HIV-infected adults receiving effective antiretroviral therapy (ART) fails to normalize this ratio, even after they achieve normal CD4+ T cell counts. The immunologic and clinical characteristics of this clinical phenotype remain undefined. Using data from four distinct clinical cohorts and three clinical trials, we show that a low CD4/CD8 ratio in HIV-infected adults during otherwise effective ART (after CD4 count recovery above 500 cells/mm3) is associated with a number of immunological abnormalities, including a skewed T cell phenotype from naïve toward terminally differentiated CD8+ T cells, higher levels of CD8+ T cell activation (HLADR+CD38+) and senescence (CD28- and CD57+CD28-), and higher kynurenine/tryptophan ratio. Changes in the peripheral CD4/CD8 ratio are also reflective of changes in gut mucosa, but not in lymph nodes. In a longitudinal study, individuals who initiated ART within six months of infection had greater CD4/CD8 ratio increase compared to later initiators (>2 years). After controlling for age, gender, ART duration, nadir and CD4 count, the CD4/CD8 ratio predicted increased risk of morbidity and mortality. Hence, a persistently low CD4/CD8 ratio during otherwise effective ART is associated with increased innate and adaptive immune activation, an immunosenescent phenotype, and higher risk of morbidity/mortality. This ratio may prove useful in monitoring response to ART and could identify a unique subset of individuals needed of novel therapeutic interventions.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- Lohse N, Hansen AB, Pedersen G, Kronborg G, Gerstoft J, et al. (2007) Survival of persons with and without HIV infection in Denmark, 1995–2005. Ann Intern Med 146: 87–95. - PubMed
-
- Bhaskaran K, Hamouda O, Sannes M, Boufassa F, Johnson AM, et al. (2008) Changes in the risk of death after HIV seroconversion compared with mortality in the general population. JAMA 300: 51–59 Available: http://www.ncbi.nlm.nih.gov/pubmed/18594040. Accessed 22 October 2013. - PubMed
-
- Zwahlen M, Harris R, May M, Hogg R, Costagliola D, et al. (2009) Mortality of HIV-infected patients starting potent antiretroviral therapy: comparison with the general population in nine industrialized countries. Int J Epidemiol 38: 1624–1633 Available: http://www.pubmedcentral.nih.gov/articlerender.fcgi?artid=3119390&tool=p.... Accessed 27 August 2013. - PMC - PubMed
-
- Guaraldi G, Orlando G, Zona S, Menozzi M, Carli F, et al. (2011) Premature age-related comorbidities among HIV-infected persons compared with the general population. Clin Infect Dis 53: 1120–1126 Available: http://www.ncbi.nlm.nih.gov/pubmed/21998278. Accessed 20 April 2013. - PubMed
-
- Deeks SG, Tracy R, Douek DC (2013) Systemic Effects of Inflammation on Health during Chronic HIV Infection. Immunity 39: 633–645 Available: http://linkinghub.elsevier.com/retrieve/pii/S1074761313004354. Accessed 18 October 2013. - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- P30 MH062246/MH/NIMH NIH HHS/United States
- P01 AI071713/AI/NIAID NIH HHS/United States
- P01 AI076174/AI/NIAID NIH HHS/United States
- K23 CA157929/CA/NCI NIH HHS/United States
- U19 AI096109/AI/NIAID NIH HHS/United States
- K24 AI069994/AI/NIAID NIH HHS/United States
- UL1 RR024131/RR/NCRR NIH HHS/United States
- U19 AI0961090/AI/NIAID NIH HHS/United States
- R01 MH54907/MH/NIMH NIH HHS/United States
- R24 AI067039/AI/NIAID NIH HHS/United States
- R21 AI087035/AI/NIAID NIH HHS/United States
- R01 AI087145/AI/NIAID NIH HHS/United States
- U10 EY008057/EY/NEI NIH HHS/United States
- R21 AI078774/AI/NIAID NIH HHS/United States
- UL1 TR000004/TR/NCATS NIH HHS/United States
- P30 MH62246/MH/NIMH NIH HHS/United States
- P01AI076174/AI/NIAID NIH HHS/United States
- R01 MH054907/MH/NIMH NIH HHS/United States
- P30 AI027763/AI/NIAID NIH HHS/United States
- R56 AI100765/AI/NIAID NIH HHS/United States
- R01 AI057020/AI/NIAID NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
