

Thrombus imaging in acute stroke: correlation of thrombus length on susceptibility-weighted imaging with endovascular reperfusion success
- PMID: 24832928
- PMCID: PMC4082654
- DOI: 10.1007/s00330-014-3200-3
Thrombus imaging in acute stroke: correlation of thrombus length on susceptibility-weighted imaging with endovascular reperfusion success
Abstract
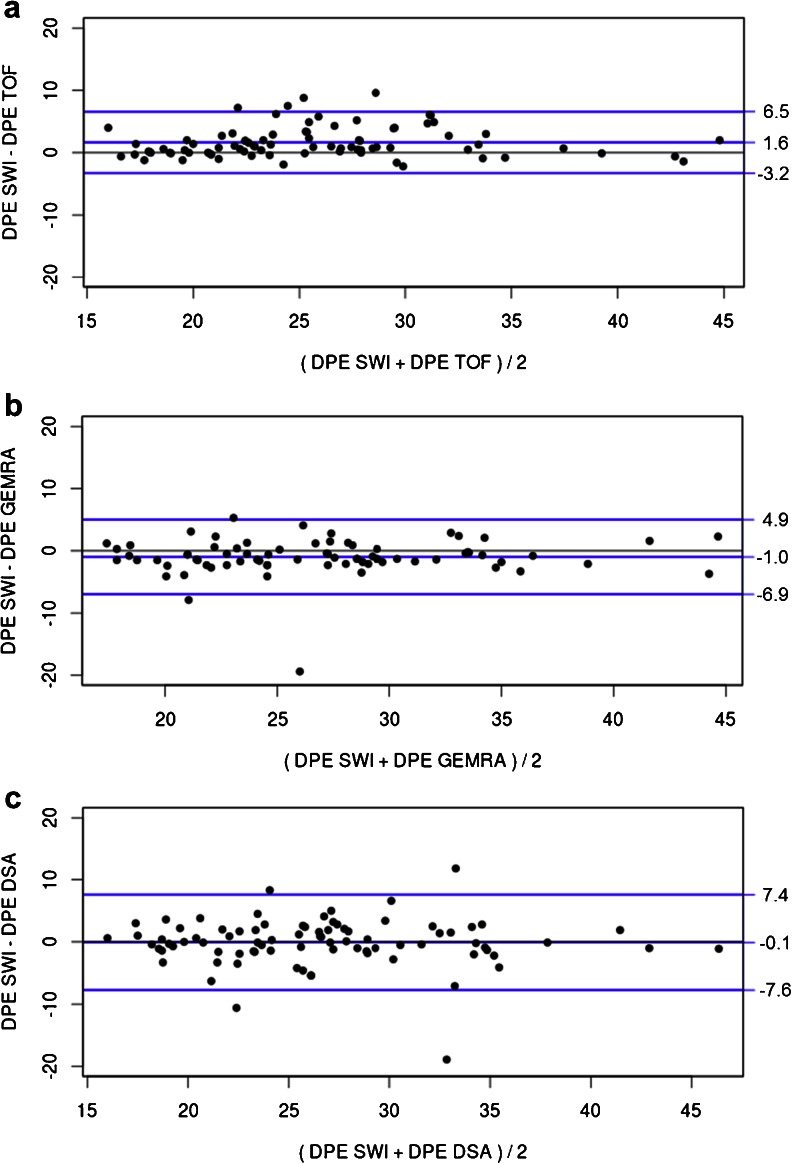
Objectives: Susceptibility-weighted imaging (SWI) enables visualization of thrombotic material in acute ischemic stroke. We aimed to validate the accuracy of thrombus depiction on SWI compared to time-of-flight MRA (TOF-MRA), first-pass gadolinium-enhanced MRA (GE-MRA) and digital subtraction angiography (DSA). Furthermore, we analysed the impact of thrombus length on reperfusion success with endovascular therapy.
Methods: Consecutive patients with acute ischemic stroke due to middle cerebral artery (MCA) occlusions undergoing endovascular recanalization were screened. Only patients with a pretreatment SWI were included. Thrombus visibility and location on SWI were compared to those on TOF-MRA, GE-MRA and DSA. The association between thrombus length on SWI and reperfusion success was studied.
Results: Eighty-four of the 88 patients included (95.5%) showed an MCA thrombus on SWI. Strong correlations between thrombus location on SWI and that on TOF-MRA (Pearson's correlation coefficient 0.918, P < 0.001), GE-MRA (0.887, P < 0.001) and DSA (0.841, P < 0.001) were observed. Successful reperfusion was not significantly related to thrombus length on SWI (P = 0.153; binary logistic regression).
Conclusions: In MCA occlusion thrombus location as seen on SWI correlates well with angiographic findings. In contrast to intravenous thrombolysis, thrombus length appears to have no impact on reperfusion success of endovascular therapy.
Key points: • SWI helps in assessing location and length of thrombi in the MCA • SWI, MRA and DSA are equivalent in detecting the MCA occlusion site • SWI is superior in identifying the distal end of the thrombus • Stent retrievers should be deployed over the distal thrombus end • Thrombus length did not affect success of endovascular reperfusion guided by SWI.
Figures



References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
