

Utilization and costs of medications associated with CKD mineral and bone disorder in dialysis patients enrolled in Medicare Part D
- PMID: 24833203
- PMCID: PMC4209315
- DOI: 10.1053/j.ajkd.2014.04.014
Utilization and costs of medications associated with CKD mineral and bone disorder in dialysis patients enrolled in Medicare Part D
Abstract
Background: Information is limited regarding utilization patterns and costs for chronic kidney disease-mineral and bone disorder (CKD-MBD) medications in Medicare Part D-enrolled dialysis patients.
Study design: Retrospective cohort study.
Setting & participants: Annual cohorts of dialysis patients, 2007-2010.
Predictors: Cohort year, low-income subsidy status, and dialysis provider.
Outcomes: Utilization and costs of prescription phosphate binders, oral and intravenous vitamin D analogues, and cinacalcet.
Measurements: Using logistic regression, we calculated adjusted odds of medication use for low-income subsidy versus non-low-income subsidy patients and for patients from various dialysis organizations, and we report per-member-per-month and average out-of-pocket costs.
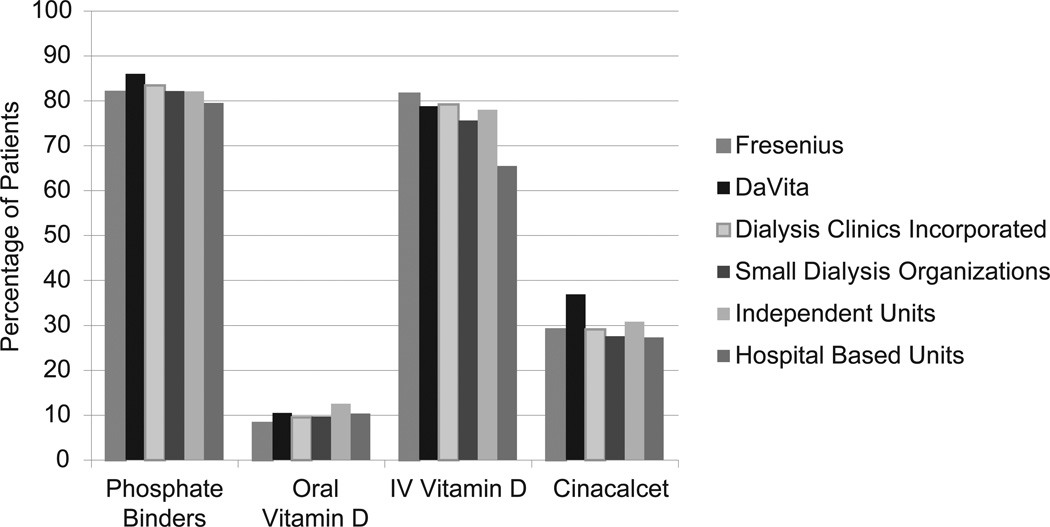
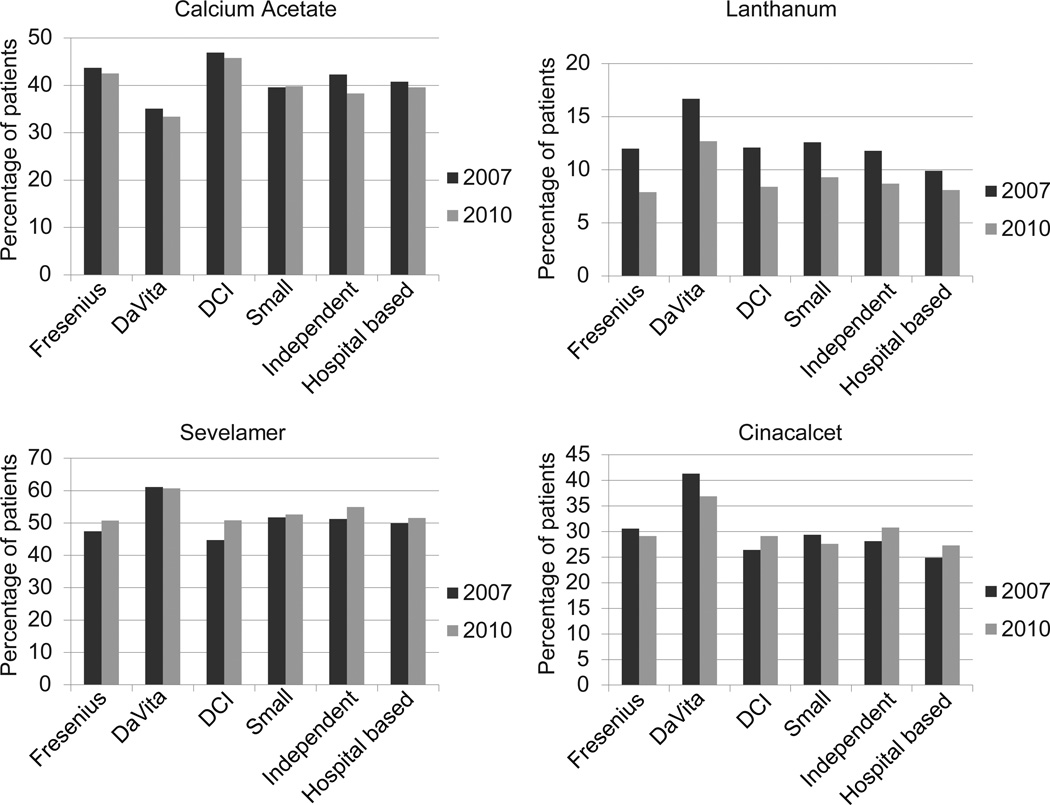
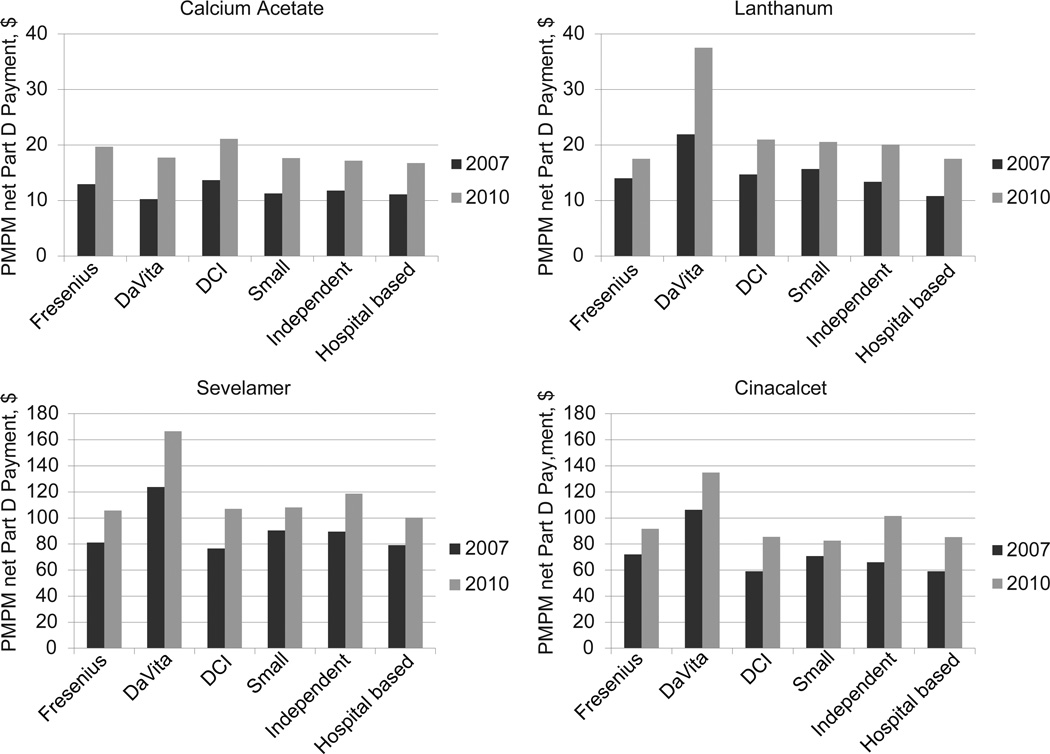
Results: Phosphate binders (∼83%) and intravenous vitamin D (77.5%-79.3%) were the most commonly used CKD-MBD medications in 2007 through 2010. The adjusted odds of prescription phosphate-binder, intravenous vitamin D, and cinacalcet use were significantly higher for low-income subsidy than for non-low-income subsidy patients. Total Part D versus CKD-MBD Part D medication costs increased 22% versus 36% from 2007 to 2010. For Part D-enrolled dialysis patients, CKD-MBD medications represented ∼50% of overall net Part D costs in 2010.
Limitations: Inability to describe utilization and costs of calcium carbonate, an over-the-counter agent not covered under Medicare Part D; inability to reliably identify prescriptions filled through a non-Part D reimbursement or payment mechanism; findings may not apply to dialysis patients without Medicare Part D benefits or with Medicare Advantage plans, or to pediatric dialysis patients; could identify only prescription drugs dispensed in the outpatient setting; inability to adjust for MBD laboratory values.
Conclusions: Part D net costs for CKD-MBD medications increased at a faster rate than costs for all Part D medications in dialysis patients despite relatively stable use within medication classes. In a bundled environment, there may be incentives to shift to generic phosphate binders and reduce cinacalcet use.
Keywords: Chronic kidney disease (CKD); Medicare Part D; calcimimetics; dialysis; medication costs; mineral and bone disorder; phosphate binders; vitamin D analogues.
Copyright © 2014 National Kidney Foundation, Inc. All rights reserved.
Figures
Similar articles
-
Adherence and persistence to prescribed medication therapy among Medicare part D beneficiaries on dialysis: comparisons of benefit type and benefit phase.J Manag Care Spec Pharm. 2014 Aug;20(8):862-76. doi: 10.18553/jmcp.2014.20.8.862. J Manag Care Spec Pharm. 2014. PMID: 25062080 Free PMC article.
-
Utilization and costs of cardiovascular disease medications in dialysis patients in Medicare Part D.Am J Kidney Dis. 2012 May;59(5):670-81. doi: 10.1053/j.ajkd.2011.10.047. Epub 2011 Dec 28. Am J Kidney Dis. 2012. PMID: 22206743
-
Trends of elevated parathormone serum titers in hemodialysis patients on intensive therapy for bone disease: a multicenter study.Saudi J Kidney Dis Transpl. 2014 Nov;25(6):1166-77. doi: 10.4103/1319-2442.144249. Saudi J Kidney Dis Transpl. 2014. PMID: 25394432
-
Impact of Cinacalcet and Etelcalcetide on Bone Mineral and Cardiovascular Disease in Dialysis Patients.Curr Osteoporos Rep. 2023 Apr;21(2):193-204. doi: 10.1007/s11914-023-00782-x. Epub 2023 Feb 27. Curr Osteoporos Rep. 2023. PMID: 36848027 Review.
-
[CKD-MBD (Chronic Kidney Disease-Mineral and Bone Disorder). Role of cinacalcet in the treatment of CKD-MBD].Clin Calcium. 2010 Jul;20(7):1089-95. Clin Calcium. 2010. PMID: 20585188 Review. Japanese.
Cited by
-
Medicare Part D's Effects on Drug Utilization and Out-of-Pocket Costs: A Systematic Review.Health Serv Res. 2017 Oct;52(5):1685-1728. doi: 10.1111/1475-6773.12534. Epub 2016 Aug 1. Health Serv Res. 2017. PMID: 27480577 Free PMC article.
-
Calcimimetic Use in Dialysis-Dependent Medicare Fee-for-Service Beneficiaries and Implications for Bundled Payment.Kidney360. 2020 Aug 25;1(10):1091-1098. doi: 10.34067/KID.0003042020. eCollection 2020 Oct 29. Kidney360. 2020. PMID: 35368776 Free PMC article.
-
Parathyroidectomy Versus Cinacalcet for the Treatment of Secondary Hyperparathyroidism in Hemodialysis Patients.World J Surg. 2022 Apr;46(4):813-819. doi: 10.1007/s00268-022-06439-7. Epub 2022 Jan 12. World J Surg. 2022. PMID: 35022799 Free PMC article.
-
Tip-toeing toward the finish line.Nephrol Dial Transplant. 2015 Jan;30(1):1-3. doi: 10.1093/ndt/gfu360. Epub 2014 Nov 20. Nephrol Dial Transplant. 2015. PMID: 25414374 Free PMC article. No abstract available.
-
Evidence basis for integrated management of mineral metabolism in patients with end-stage renal disease.Curr Opin Nephrol Hypertens. 2018 Jul;27(4):258-267. doi: 10.1097/MNH.0000000000000417. Curr Opin Nephrol Hypertens. 2018. PMID: 29677006 Free PMC article. Review.
References
-
- KDIGO CKD-MBD Workgroup. KDIGO clinical practice guideline for the diagnosis, evaluation, prevention, and treatment of Chronic Kidney Disease-Mineral and Bone Disorder (CKD-MBD) Kidney Int. 2009;76(suppl 113):S1–S130. - PubMed
-
- Moe SM, Drueke T, Lameire N, Eknoyan G. Chronic kidney disease-mineral-bone disorder: a new paradigm. Adv Chronic Kidney Dis. 2007;14(1):3–12. - PubMed
-
- U.S. Renal Data System. USRDS 2012 Annual Data Report: Atlas of Chronic Kidney Disease & End-Stage Renal Disease in the United States. Bethesda, MD: National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases; 2012.
-
- Pai AB, Shepler BM. Comparison of sevelamer hydrochloride and sevelamer carbonate: risk of metabolic acidosis and clinical implications. Pharmacotherapy. 2009;29(5):554–561. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
