

Bacterial biofilms on implanted suture material are a cause of surgical site infection
- PMID: 24833403
- PMCID: PMC4195429
- DOI: 10.1089/sur.2013.016
Bacterial biofilms on implanted suture material are a cause of surgical site infection
Abstract
Background: Surgical site infection (SSI) has been estimated to occur in up to 5% of all procedures, accounting for up to 0.5% of all hospital costs. Bacterial biofilms residing on implanted foreign bodies have been implicated as contributing or causative factors in a wide variety of infectious scenarios, but little consideration has been given to the potential for implanted, submerged suture material to act as a host for biofilm and thus serve as a nidus of infection.
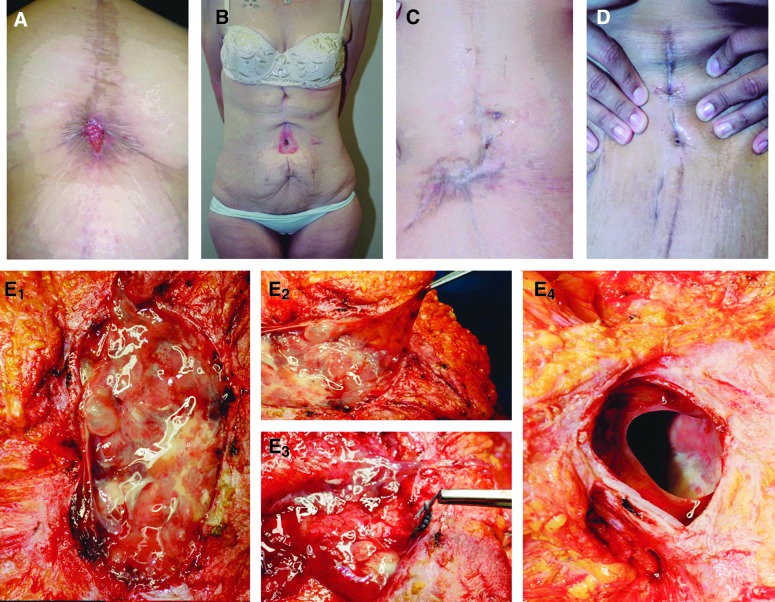
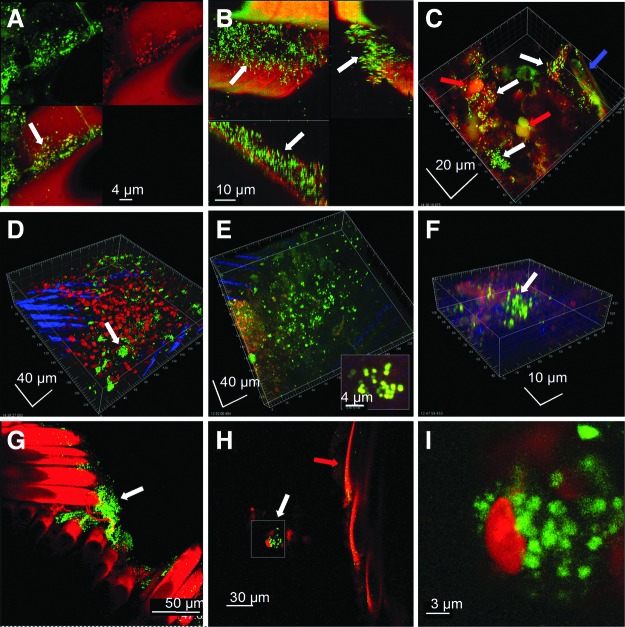
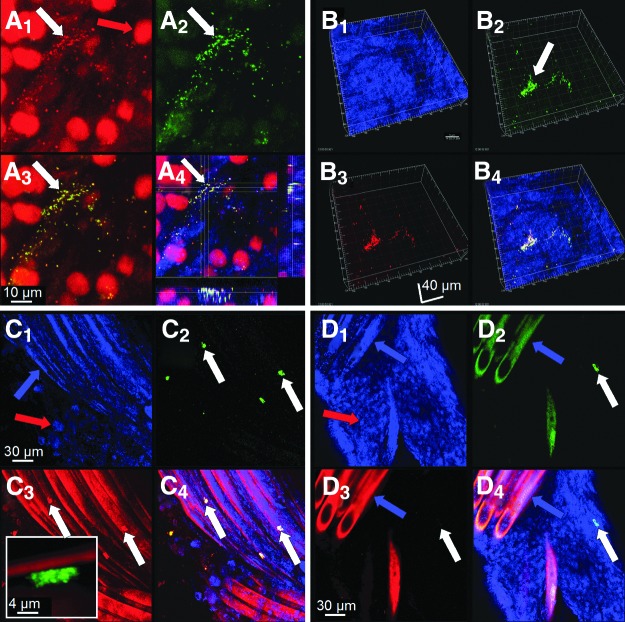
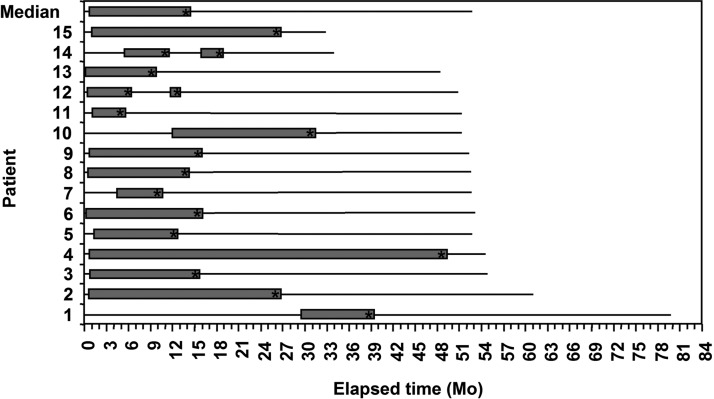
Methods: We report a series of 15 patients who underwent open Roux-en-Y gastric bypass (with musculofascial closure with permanent, multifilament sutures) who developed longstanding and refractory SSIs in the abdominal wall. Explanted suture material at subsequent exploration was examined for biofilm with confocal laser-scanning microscopy (CLSM) and fluorescence in situ hybridization (FISH).
Results: All 15 patients at re-exploration were found to have gross evidence of a "slimy" matrix or dense reactive granulation tissue localized to the implanted sutures. Confocal laser-scanning microscopy revealed abundant biofilm present on all sutures examined; FISH was able to identify the presence of specific pathogens in the biofilm. Complete removal of the foreign bodies (and attendant biofilms) resulted in all cases in cure of the SSI.
Conclusion: Bacterial biofilms on implanted suture material can manifest as persistent surgical site infections that require complete removal of the underlying foreign body substrata for resolution.
Figures
References
-
- Cheadle WG. Risk factors for surgical site infection. Surg Infect (Larchmt) 2006;7Suppl 1:S7–S11 - PubMed
-
- Fry DE. The economic costs of surgical site infection. Surg Infect (Larchmt) 2002;3Suppl 1:S37–S43 - PubMed
-
- Edmiston CE, Seabrook GR, Goheen MP, et al. . Bacterial adherence to surgical sutures: Can antibacterial-coated sutures reduce the risk of microbial contamination? J Am Coll Surg 2006;203:481–489 - PubMed
-
- Turina M, Cheadle WG. Management of established surgical site infections. Surg Infect (Larchmt) 2006; 7Suppl 3:S33–S41 - PubMed
-
- Rasnake MS, Dooley DP. Culture-negative surgical site infections. Surg Infect (Larchmt) 2006;7:555–565 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
