

Feasibility study of stereotactic body radiotherapy for peripheral lung tumors with a maximum dose of 100 Gy in five fractions and a heterogeneous dose distribution in the planning target volume
- PMID: 24833770
- PMCID: PMC4202295
- DOI: 10.1093/jrr/rru037
Feasibility study of stereotactic body radiotherapy for peripheral lung tumors with a maximum dose of 100 Gy in five fractions and a heterogeneous dose distribution in the planning target volume
Abstract
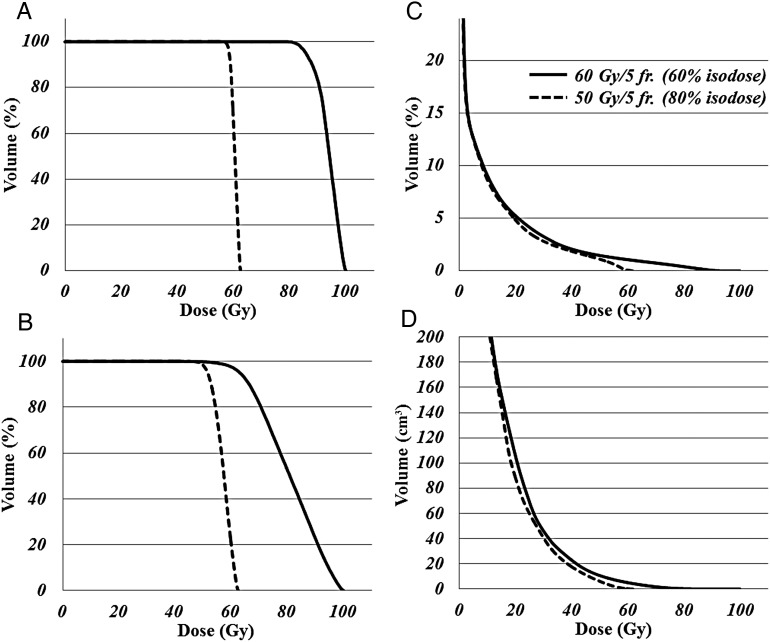
We evaluated toxicity and outcomes for patients with peripheral lung tumors treated with stereotactic body radiation therapy (SBRT) in a dose-escalation and dose-convergence study. A total of 15 patients were enrolled. SBRT was performed with 60 Gy in 5 fractions (fr.) prescribed to the 60% isodose line of maximum dose, which was 100 Gy in 5 fr., covering the planning target volume (PTV) surface (60 Gy/5 fr. - (60%-isodose)) using dynamic conformal multiple arc therapy (DCMAT). The primary endpoint was radiation pneumonitis (RP) ≥ Grade 2 within 6 months. Toxicities were graded according to the Common Terminology Criteria for Adverse Events, version 4.0. Using dose-volumetric analysis, the trial regimen of 60 Gy/5 fr. - (60%-isodose) was compared with our institutional conventional regimen of 50 Gy/5 fr. - (80%-isodose). The enrolled consecutive patients had either a solitary peripheral tumor or two ipsilateral tumors. The median follow-up duration was 22.0 (12.0-27.0) months. After 6 months post-SBRT, the respective number of RP Grade 0, 1 and 2 cases was 5, 9 and 1. In the Grade 2 RP patient, the image showed an organizing pneumonia pattern at 6.0 months post-SBRT. No other toxicity was found. At last follow-up, there was no evidence of recurrence of the treated tumors. The target volumes of 60 Gy/ 5 fr. - (60%-isodose) were irradiated with a significantly higher dose than those of 50 Gy/5 fr. - (80%-isodose), while the former dosimetric parameters of normal lung were almost equivalent to the latter. SBRT with 60 Gy/5 fr. - (60%-isodose) using DCMAT allowed the delivery of very high and convergent doses to peripheral lung tumors with feasibility in the acute and subacute phases. Further follow-up is required to assess for late toxicity.
Keywords: Phase I study; dose-escalation study; homogeneity index; lung cancer; prescription dose; stereotactic body ridiotherapy.
© The Author 2014. Published by Oxford University Press on behalf of The Japan Radiation Research Society and Japanese Society for Radiation Oncology.
Figures

Similar articles
-
Dose distribution analysis in stereotactic body radiotherapy using dynamic conformal multiple arc therapy.Int J Radiat Oncol Biol Phys. 2009 Jun 1;74(2):363-9. doi: 10.1016/j.ijrobp.2008.08.012. Int J Radiat Oncol Biol Phys. 2009. PMID: 19427552
-
Assessment of Monte Carlo algorithm for compliance with RTOG 0915 dosimetric criteria in peripheral lung cancer patients treated with stereotactic body radiotherapy.J Appl Clin Med Phys. 2016 May 8;17(3):277-293. doi: 10.1120/jacmp.v17i3.6077. J Appl Clin Med Phys. 2016. PMID: 27167284 Free PMC article.
-
Toxicity after central versus peripheral lung stereotactic body radiation therapy: a propensity score matched-pair analysis.Int J Radiat Oncol Biol Phys. 2015 Jan 1;91(1):124-32. doi: 10.1016/j.ijrobp.2014.08.345. Epub 2014 Oct 18. Int J Radiat Oncol Biol Phys. 2015. PMID: 25442337
-
Stereotactic body radiotherapy for Ultra-Central lung Tumors: A systematic review and Meta-Analysis and International Stereotactic Radiosurgery Society practice guidelines.Lung Cancer. 2023 Aug;182:107281. doi: 10.1016/j.lungcan.2023.107281. Epub 2023 Jun 21. Lung Cancer. 2023. PMID: 37393758
-
Stereotactic body radiotherapy for intramedullary metastases: a retrospective series at the Oscar Lambret center and a systematic review.BMC Cancer. 2021 Oct 30;21(1):1168. doi: 10.1186/s12885-021-08901-6. BMC Cancer. 2021. PMID: 34717570 Free PMC article.
Cited by
-
Stereotactic body radiotherapy for patients with oligometastases from colorectal cancer: risk-adapted dose prescription with a maximum dose of 83-100 Gy in five fractions.J Radiat Res. 2016 Jul;57(4):400-5. doi: 10.1093/jrr/rrw029. Epub 2016 Mar 16. J Radiat Res. 2016. PMID: 26983981 Free PMC article.
-
Simple Factors Associated With Radiation-Induced Lung Toxicity After Stereotactic Body Radiation Therapy of the Thorax: A Pooled Analysis of 88 Studies.Int J Radiat Oncol Biol Phys. 2016 Aug 1;95(5):1357-1366. doi: 10.1016/j.ijrobp.2016.03.024. Epub 2016 Mar 25. Int J Radiat Oncol Biol Phys. 2016. PMID: 27325482 Free PMC article. Review.
-
Treatment-Related Adverse Effects in Lung Cancer Patients after Stereotactic Ablative Radiation Therapy.J Oncol. 2018 Oct 4;2018:6483626. doi: 10.1155/2018/6483626. eCollection 2018. J Oncol. 2018. PMID: 30402100 Free PMC article. Review.
-
A phase I/II study on stereotactic body radiotherapy with real-time tumor tracking using CyberKnife based on the Monte Carlo algorithm for lung tumors.Int J Clin Oncol. 2017 Aug;22(4):706-714. doi: 10.1007/s10147-017-1123-0. Epub 2017 Apr 20. Int J Clin Oncol. 2017. PMID: 28429140 Clinical Trial.
-
Assessment of biological dosimetric margin for stereotactic body radiation therapy.J Appl Clin Med Phys. 2020 Apr;21(4):31-41. doi: 10.1002/acm2.12843. Epub 2020 Mar 6. J Appl Clin Med Phys. 2020. PMID: 32141684 Free PMC article.
References
-
- Ettinger DS, Akerley W, Borghaei H, et al. NCCN Clinical Practice Guidelines in Oncology website. Non-small cell lung cancer, version 2.2013. National Comprehensive Cancer Network, 2013. http://www.nccn.org/professionals/physician_gls/f_guidelines.asp. (13 September 2013, date last accessed)
-
- Takeda A, Kunieda E, Ohashi T, et al. Stereotactic body radiotherapy (SBRT) for oligometastatic lung tumors from colorectal cancer and other primary cancers in comparison with primary lung cancer. Radiother Oncol. 2011;101:255–9. - PubMed
-
- Norihisa Y, Nagata Y, Takayama K, et al. Stereotactic body radiotherapy for oligometastatic lung tumors. Int J Radiat Oncol Biol Phys. 2008;72:398–403. - PubMed
-
- Takeda A, Kunieda E, Sanuki N, et al. Dose distribution analysis in stereotactic body radiotherapy using dynamic conformal multiple arc therapy. Int J Radiat Oncol Biol Phys. 2009;74:363–9. - PubMed
-
- Takeda A, Sanuki N, Kunieda E, et al. Stereotactic body radiotherapy for primary lung cancer at a dose of 50 Gy total in five fractions to the periphery of the planning target volume calculated using a superposition algorithm. Int J Radiat Oncol Biol Phys. 2009;73:442–8. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
