

Colorectal cancer and immunity: what we know and perspectives
- PMID: 24833840
- PMCID: PMC3983433
- DOI: 10.3748/wjg.v20.i14.3738
Colorectal cancer and immunity: what we know and perspectives
Abstract
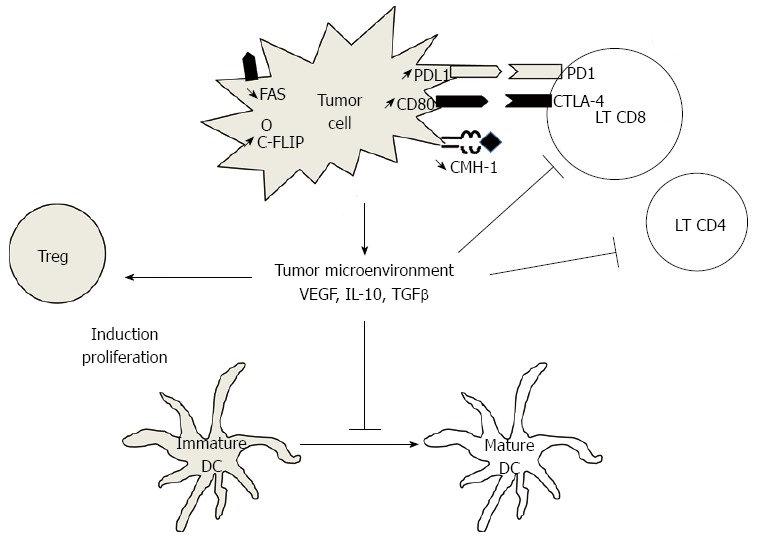
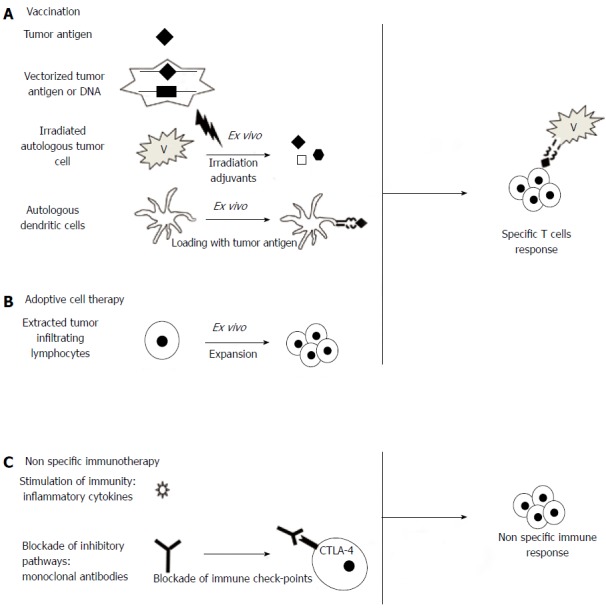
Strong evidence supports the concept of immunosurveillance and immunoediting in colorectal cancer. In particular, the density of T CD8⁺ and CD45⁺ lymphocyte infiltration was recently shown to have a better prognostic value than the classic tumor node metastasis classification factor. Other immune subsets, as macrophages, natural killer cells or unconventionnal lymphocytes, seem to play an important role. Induction of regulatory T cells (Tregs) or immunosuppressive molecules such as PD-1 or CTLA-4 and downregulation of antigen-presenting molecules are major escape mechanisms to antitumor immune response. The development of these mechanisms is a major obstacle to the establishment of an effective immune response, but also to the use of immunotherapy. Although immunotherapy is not yet routinely used in colorectal cancer, we now know that most treatments used (chemotherapy and biotherapy) have immunomodulatory effects, such as induction of immunogenic cell death by chemotherapy, inhibition of immunosuppression by antiangiogenic agents, and antibody-dependent cytotoxicity induced by cetuximab. Finally, many immunotherapy strategies are being developed and tested in phase I to III clinical trials. The most promising strategies are boosting the immune system with cytokines, inhibition of immunoregulatory checkpoints, vaccination with vectorized antigens, and adoptive cell therapy. Comprehension of antitumor immune response and combination of the different approaches of immunotherapy may allow the use of effective immunotherapy for treatment of colorectal cancer in the near future.
Keywords: Colorectal cancer; Immunity; Immunoregulation; Immunotherapy; Vaccination.
Figures
References
-
- Pham SM, Kormos RL, Landreneau RJ, Kawai A, Gonzalez-Cancel I, Hardesty RL, Hattler BG, Griffith BP. Solid tumors after heart transplantation: lethality of lung cancer. Ann Thorac Surg. 1995;60:1623–1626. - PubMed
-
- Frisch M, Biggar RJ, Engels EA, Goedert JJ. Association of cancer with AIDS-related immunosuppression in adults. JAMA. 2001;285:1736–1745. - PubMed
-
- Collett D, Mumford L, Banner NR, Neuberger J, Watson C. Comparison of the incidence of malignancy in recipients of different types of organ: a UK Registry audit. Am J Transplant. 2010;10:1889–1896. - PubMed
-
- Grulich AE, van Leeuwen MT, Falster MO, Vajdic CM. Incidence of cancers in people with HIV/AIDS compared with immunosuppressed transplant recipients: a meta-analysis. Lancet. 2007;370:59–67. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
