

Usefulness of MRI in takotsubo cardiomyopathy: a review of the literature
- PMID: 24834411
- PMCID: PMC3996242
- DOI: 10.3978/j.issn.2223-3652.2013.10.03
Usefulness of MRI in takotsubo cardiomyopathy: a review of the literature
Abstract
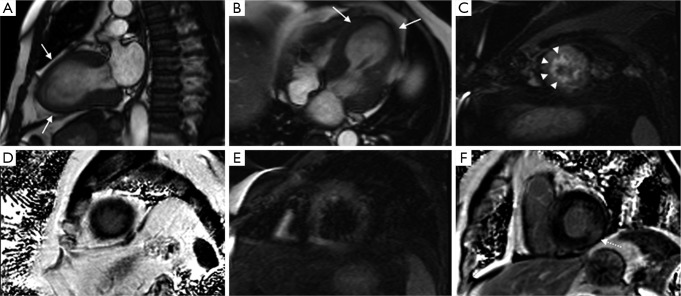
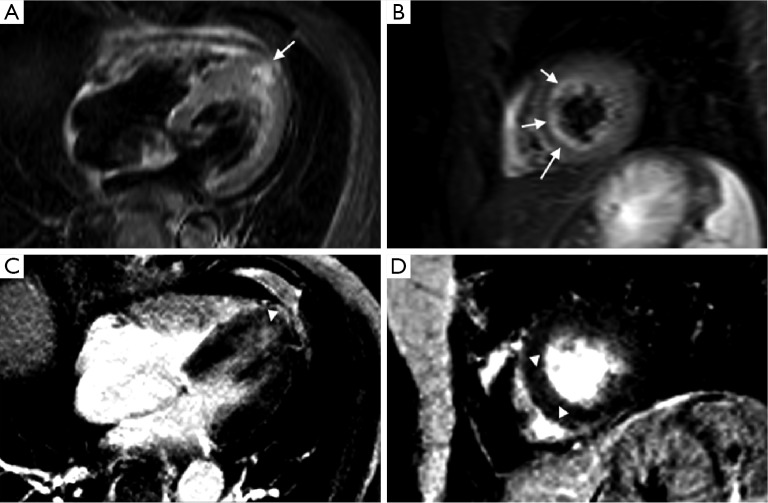
Takotsubo cardiomyopathy (TC) is a disease that can be misinterpreted as a more serious acute coronary syndrome. Its clinical characteristics resemble those of a myocardial infarct, while its imaging characteristics are critical on correctly characterizing and diagnosing the disease. From angiography, where coronary anatomy is evaluated, to cardiac magnetic resonance (CMR), where morphology and tissue characterization is assessed, the array of imaging options is quite extent. In particular, CMR has achieved great improvements (stronger magnetic fields, better coils, etc.) in the last decade which in turn has made this imaging technology more attractive in the evaluation and diagnosis of TC. With its superior soft tissue resolution and dynamic imaging capabilities, CMR is currently, perhaps, the most useful imaging technique in TC as apical ballooning or medio-basal wall motion abnormalities (WMA), presence of wall edema and late gadolinium enhancement (LGE) characteristics are critical in the diagnosis and characterization of this pathology. In this review, CMRs role in TC will be evaluated in light of the current available evidence in medical literature, while also revising the clinical and physiopathologic characteristics of TC.
Keywords: Broken heart syndrome; MRI; chest pain; reversible cardiomyopathy; stress cardiomyopathy; takotsubo.
Figures
Similar articles
-
Advanced cardiac magnetic resonance imaging in takotsubo cardiomyopathy.Br J Radiol. 2020 Nov 1;93(1115):20200514. doi: 10.1259/bjr.20200514. Epub 2020 Aug 14. Br J Radiol. 2020. PMID: 32795180 Free PMC article. Review.
-
Takotsubo Cardiomyopathy: Role of Cardiac MRI.J Radiol Case Rep. 2021 Jun 30;15(6):26-32. doi: 10.3941/jrcr.v15i6.4138. eCollection 2021 Jun. J Radiol Case Rep. 2021. PMID: 34276878 Free PMC article.
-
Prevalence and signal characteristics of late gadolinium enhancement on contrast-enhanced magnetic resonance imaging in patients with takotsubo cardiomyopathy.Circ J. 2012;76(4):914-21. doi: 10.1253/circj.cj-11-1043. Epub 2012 Jan 27. Circ J. 2012. PMID: 22293447
-
Morphologic pattern of late gadolinium enhancement in Takotsubo cardiomyopathy detected by early cardiovascular magnetic resonance.Clin Cardiol. 2011 Mar;34(3):178-82. doi: 10.1002/clc.20877. Clin Cardiol. 2011. PMID: 21400545 Free PMC article.
-
Biventricular takotsubo cardiomyopathy with asymmetrical wall motion abnormality between left and right ventricle: a report of new case and literature review.J Echocardiogr. 2019 Sep;17(3):123-128. doi: 10.1007/s12574-019-00424-1. Epub 2019 Mar 23. J Echocardiogr. 2019. PMID: 30905042 Review.
Cited by
-
Role of cardiac magnetic resonance imaging in identifying infarct related artery and non-ischemic pathogenesis in patients presenting with non ST elevation myocardial infarction.Indian Heart J. 2024 Mar-Apr;76(2):101-107. doi: 10.1016/j.ihj.2024.02.004. Epub 2024 Feb 24. Indian Heart J. 2024. PMID: 38408612 Free PMC article.
-
Serotonin Syndrome Induced Tako-Tsubo Syndrome.Case Rep Cardiol. 2022 Jun 26;2022:7551440. doi: 10.1155/2022/7551440. eCollection 2022. Case Rep Cardiol. 2022. PMID: 35795821 Free PMC article.
-
The Stressed Heart: A Case Report of Takotsubo Cardiomyopathy in a Patient With Known Coronary Artery Disease.Cureus. 2023 Mar 17;15(3):e36277. doi: 10.7759/cureus.36277. eCollection 2023 Mar. Cureus. 2023. PMID: 37073186 Free PMC article.
-
Advanced cardiac magnetic resonance imaging in takotsubo cardiomyopathy.Br J Radiol. 2020 Nov 1;93(1115):20200514. doi: 10.1259/bjr.20200514. Epub 2020 Aug 14. Br J Radiol. 2020. PMID: 32795180 Free PMC article. Review.
-
Recurrent Takotsubo cardiomyopathy in a postmenopausal Indian lady: Is there a pattern?J Postgrad Med. 2019 Apr-Jun;65(2):112-115. doi: 10.4103/jpgm.JPGM_383_17. J Postgrad Med. 2019. PMID: 30117480 Free PMC article.
References
-
- Dote K, Sato H, Tateishi H, et al. Myocardial stunning due to simultaneous multivessel coronary spasms: a review of 5 cases. J Cardiol 1991;21:203-14 - PubMed
-
- Pernicova I, Garg S, Bourantas CV, et al. Takotsubo cardiomyopathy: a review of the literature. Angiology 2010;61:166-73 - PubMed
-
- Bybee KA, Kara T, Prasad A, et al. Systematic review: transient left ventricular apical ballooning: a syndrome that mimics ST-segment elevation myocardial infarction. Ann Intern Med 2004;141:858-65 - PubMed
-
- Arias AM, Oberti PF, Pizarro R, et al. Dobutamine-precipitated Takotsubo cardiomyopathy mimicking acute myocardial infarction: a multimodality image approach. Circulation 2011;124:e312-5 - PubMed
Publication types
LinkOut - more resources
Full Text Sources