

4D flow imaging with MRI
- PMID: 24834414
- PMCID: PMC3996243
- DOI: 10.3978/j.issn.2223-3652.2014.01.02
4D flow imaging with MRI
Abstract
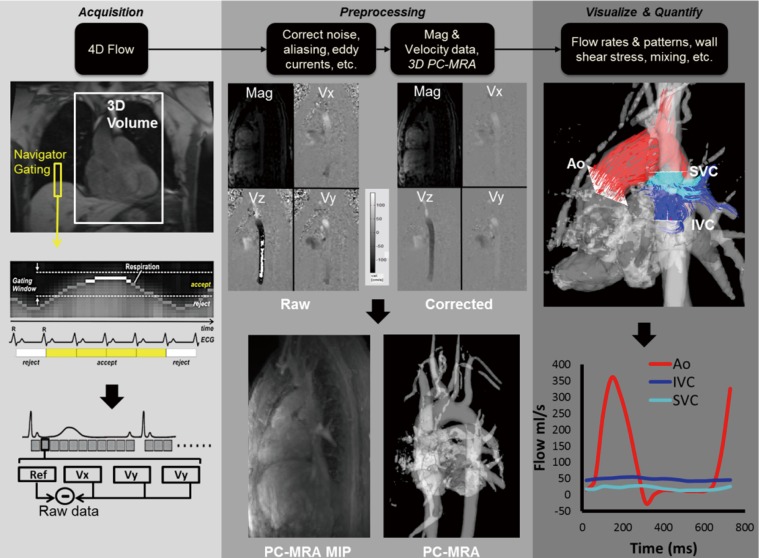
Magnetic resonance imaging (MRI) has become an important tool for the clinical evaluation of patients with cardiovascular disease. Since its introduction in the late 1980s, 2-dimensional phase contrast MRI (2D PC-MRI) has become a routine part of standard-of-care cardiac MRI for the assessment of regional blood flow in the heart and great vessels. More recently, time-resolved PC-MRI with velocity encoding along all three flow directions and three-dimensional (3D) anatomic coverage (also termed '4D flow MRI') has been developed and applied for the evaluation of cardiovascular hemodynamics in multiple regions of the human body. 4D flow MRI allows for the comprehensive evaluation of complex blood flow patterns by 3D blood flow visualization and flexible retrospective quantification of flow parameters. Recent technical developments, including the utilization of advanced parallel imaging techniques such as k-t GRAPPA, have resulted in reasonable overall scan times, e.g., 8-12 minutes for 4D flow MRI of the aorta and 10-20 minutes for whole heart coverage. As a result, the application of 4D flow MRI in a clinical setting has become more feasible, as documented by an increased number of recent reports on the utility of the technique for the assessment of cardiac and vascular hemodynamics in patient studies. A number of studies have demonstrated the potential of 4D flow MRI to provide an improved assessment of hemodynamics which might aid in the diagnosis and therapeutic management of cardiovascular diseases. The purpose of this review is to describe the methods used for 4D flow MRI acquisition, post-processing and data analysis. In addition, the article provides an overview of the clinical applications of 4D flow MRI and includes a review of applications in the heart, thoracic aorta and hepatic system.
Keywords: 4D flow magnetic resonance imaging (4D flow MRI); PC-VIPR; aorta; blood flow; carotid bifurcation; heart; hemodynamics; liver hemodynamics; peripheral arteries; phase contrast magnetic resonance imaging (PC-MRI); pulmonary arteries; quantification; renal arteries; splanchnic vessel system; visualization.
Figures








References
-
- Moran PR. A flow velocity zeugmatographic interlace for NMR imaging in humans. Magn Reson Imaging 1982;1:197-203 - PubMed
-
- Bryant DJ, Payne JA, Firmin DN, et al. Measurement of flow with NMR imaging using a gradient pulse and phase difference technique. J Comput Assist Tomogr 1984;8:588-93 - PubMed
-
- Nayler GL, Firmin DN, Longmore DB. Blood flow imaging by cine magnetic resonance. J Comput Assist Tomogr 1986;10:715-22 - PubMed
-
- Firmin DN, Nayler GL, Klipstein RH, et al. In vivo validation of MR velocity imaging. J Comput Assist Tomogr 1987;11:751-6 - PubMed
-
- Pelc NJ, Herfkens RJ, Shimakawa A, et al. Phase contrast cine magnetic resonance imaging. Magn Reson Q 1991;7:229-54 - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials