

Care transitions between hospitals are associated with treatment delay for patients with muscle invasive bladder cancer
- PMID: 24835054
- PMCID: PMC4422495
- DOI: 10.1016/j.juro.2014.05.027
Care transitions between hospitals are associated with treatment delay for patients with muscle invasive bladder cancer
Abstract
Purpose: Hypothesizing that changing hospitals between diagnosis and definitive therapy (care transition) may delay timely treatment, we identified the association between care transitions and a treatment delay of 3 months or greater in patients with muscle invasive bladder cancer.
Materials and methods: Using the National Cancer Database we identified all patients with stage II or greater urothelial carcinoma treated from 2003 to 2010. Care transition was defined as a change in hospital from diagnosis to definitive treatment course, that is diagnosis to radical cystectomy or the start of neoadjuvant chemotherapy. Logistic regression models were used to test the association between care transition and treatment delay.
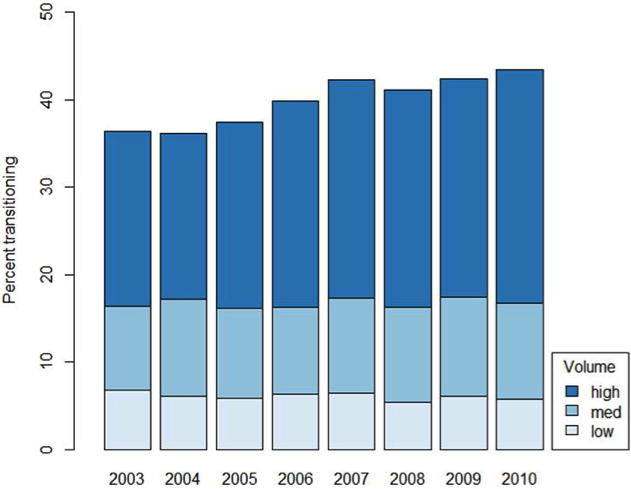
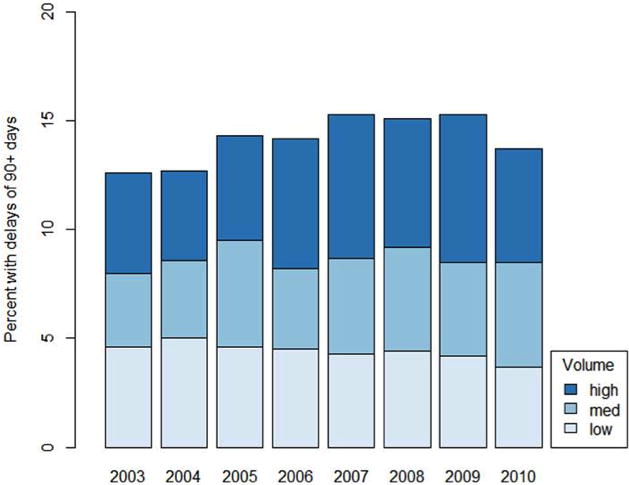
Results: Of 22,251 patients 14.2% experienced a treatment delay of 3 months or greater and this proportion increased with time (13.5% in 2003 to 2006 vs 14.8% in 2007 to 2010, p = 0.01). Of patients who underwent a care transition 19.4% experienced a delay to definitive treatment compared to 10.7% diagnosed and treated at the same hospital (p <0.001). The proportion of patients with a care transition increased during the study period (37.4% in 2003 to 2006 vs 42.3% in 2007 to 2010, p <0.001). After adjustment patients were more likely to experience a treatment delay when undergoing a care transition (OR 2.0, 95% CI 1.8-2.2).
Conclusions: Patients with muscle invasive bladder cancer who underwent a care transition were more likely to experience a treatment delay of 3 months or greater. Strategies to expedite care transitions at the time of hospital referral may improve quality of care.
Keywords: cystectomy; health care; hospitals; patient handoff; quality indicators; urinary bladder neoplasms.
Copyright © 2014 American Urological Association Education and Research, Inc. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Brock J, Mitchell J, Irby K, et al. Association between quality improvement for care transitions in communities and rehospitalizations among Medicare beneficiaries. JAMA. 2013;309:381. - PubMed
-
- Birkmeyer JD, Siewers AE, Finlayson EV, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;346:1128. - PubMed
-
- Birkmeyer JD, Dimick JB. Potential benefits of the new Leapfrog standards: effect of process and outcomes measures. Surgery. 2004;135:569. - PubMed
-
- Hollenbeck BK, Dunn RL, Miller DC, et al. Volume-based referral for cancer surgery: informing the debate. J Clin Oncol. 2007;25:91. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
