

Laparoscopic versus open radical cystectomy in bladder cancer: a systematic review and meta-analysis of comparative studies
- PMID: 24835573
- PMCID: PMC4023936
- DOI: 10.1371/journal.pone.0095667
Laparoscopic versus open radical cystectomy in bladder cancer: a systematic review and meta-analysis of comparative studies
Abstract
Background and objective: More recently laparoscopic radical cystectomy (LRC) has increasingly been an attractive alternative to open radical cystectomy (ORC) and many centers have reported their early experiences in the treatment of bladder cancer. Evaluate the safety and efficacy of LRC compared with ORC in the treatment of bladder cancer.
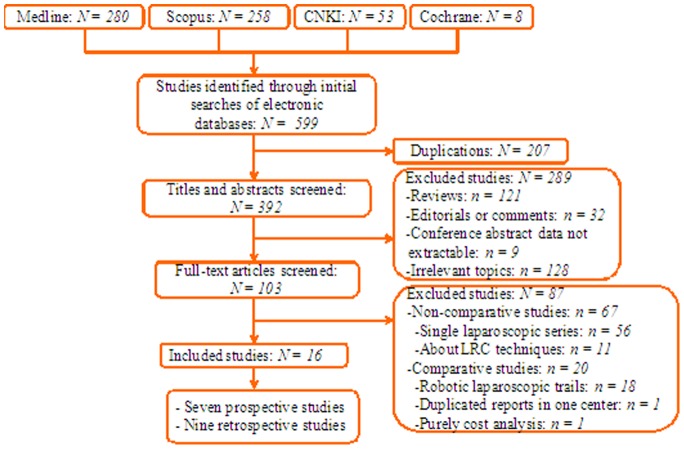
Methods: A systematic search of Medline, Scopus, and the Cochrane Library was performed up to Mar 1, 2013. Outcomes of interest assessing the two techniques included demographic and clinical baseline characteristics, perioperative, pathologic and oncological variables, and post-op neobladder function and complications.
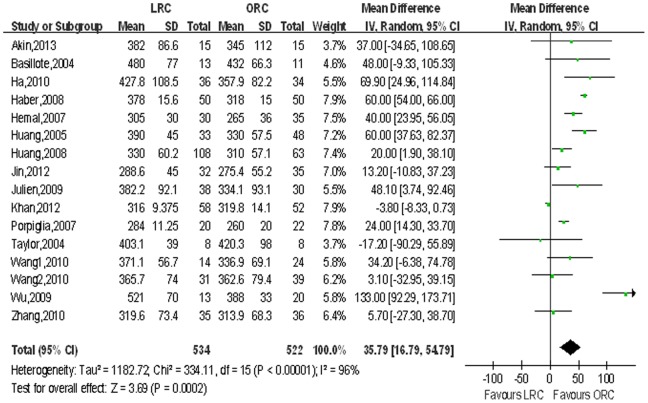
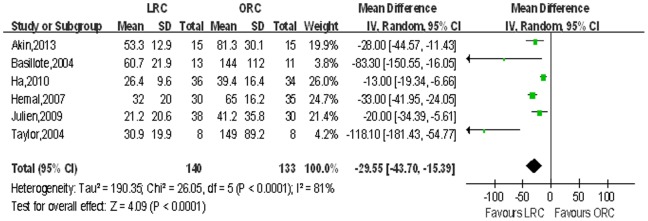
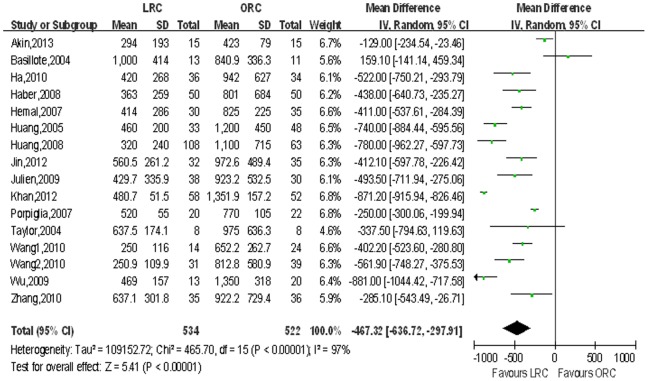
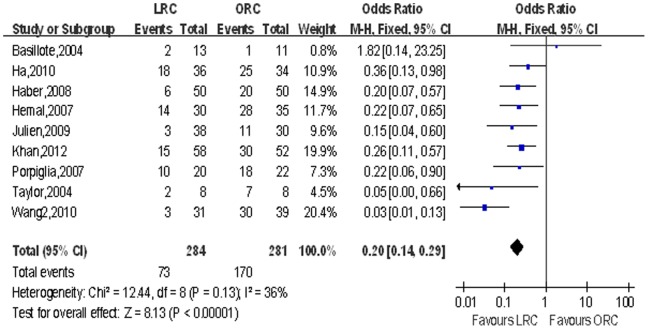
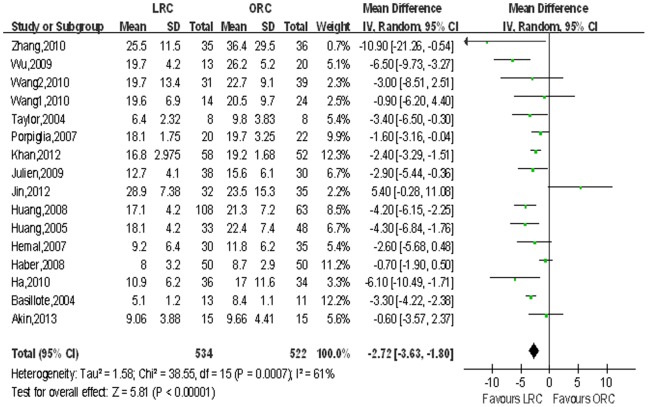
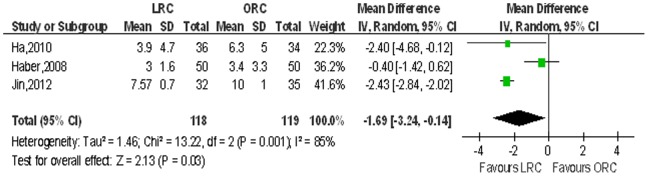
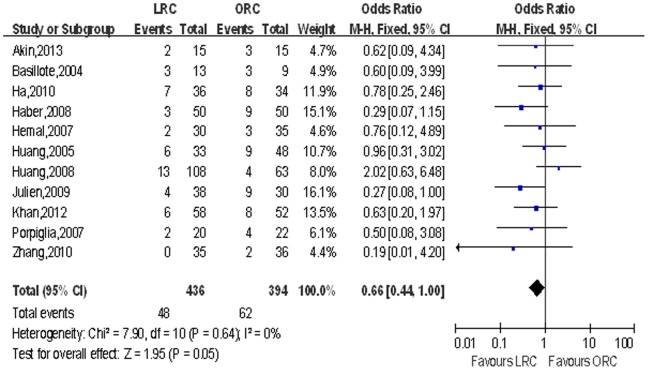
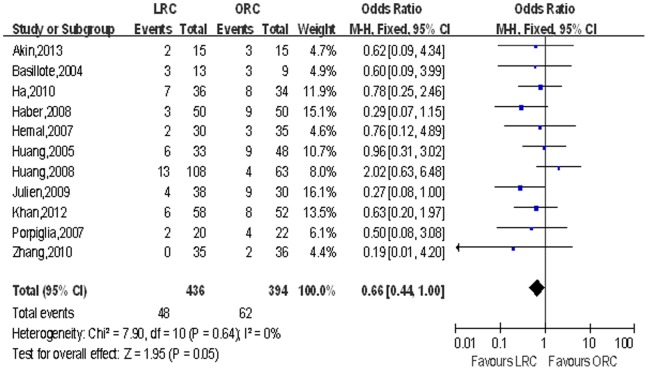
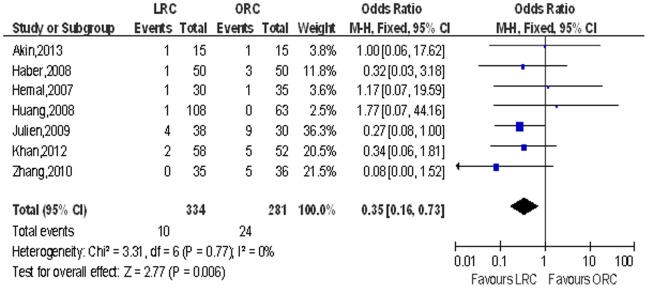
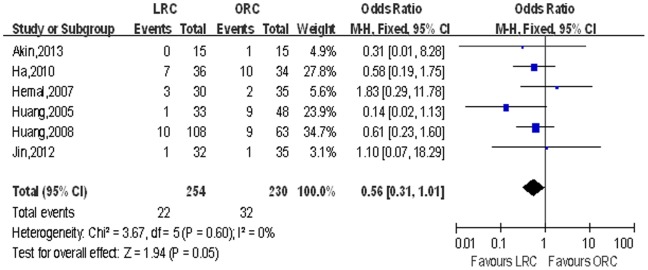
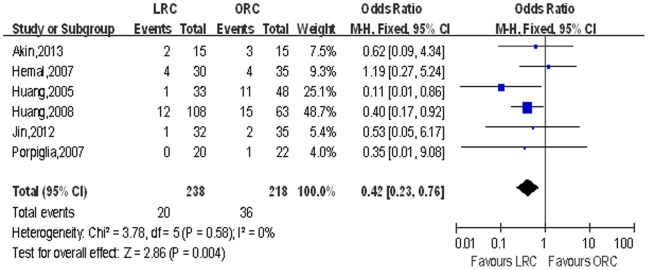
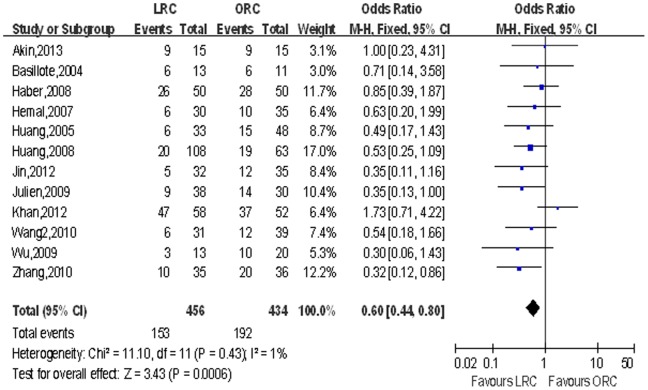
Results: Sixteen eligible trials evaluating LRC vs ORC were identified including seven prospective and nine retrospective studies. Although LRC was associated with longer operative time (p<0.001), patients might benefit from significantly fewer overall complications (p<0.001), less blood loss (p<0.001), shorter length of hospital stay (p<0.001), less need of blood transfusion (p<0.001), less narcotic analgesic requirement (p<0.001), shorter time to ambulation (p = 0.03), shorter time to regular diet (p<0.001), fewer positive surgical margins (p = 0.006), fewer positive lymph node (p = 0.05), lower distant metastasis rate (p = 0.05) and fewer death (p = 0.004). There was no significant difference in other demographic parameters except for a lower ASA score (p = 0.01) in LRC while post-op neobladder function were similar between the two groups.
Conclusions: Our data suggest that LRC appears to be a safe, feasible and minimally invasive alternative to ORC with reliable perioperative safety, pathologic & oncologic efficacy, comparable post-op neobladder function and fewer complications. Because of the inherent limitations of the included studies, further large sample prospective, multi-centric, long-term follow-up studies and randomized control trials should be undertaken to confirm our findings.
Conflict of interest statement
Figures
References
-
- Kaufman DS, Shipley WU, Feldman AS (2009) Bladder cancer. Lancet 18 374: 239–249. - PubMed
-
- Witjes JA, Compérat E, Cowan NC, De Santis M, Gakis G, et al. (2014) EAU Guidelines on Muscle-invasive and Metastatic Bladder Cancer: Summary of the 2013 Guidelines. Eur Urol 65(4): 778–792. - PubMed
-
- Fairey AS, Jacobsen NE, Chetner MP, Mador DR, Metcalfe JB, et al. (2009) Associations between comorbidity, and overall survival and bladder cancer specific survival after radical cystectomy: results from the Alberta Urology Institute Radical Cystectomy database. J Urol 182: 85–92 discussion 3. - PubMed
-
- Konety BR, Allareddy V, Herr H (2006) Complications after radical cystectomy: analysis of population-based data. Urology 68: 58–64. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
