

Review
doi: 10.1053/j.semperi.2014.03.005.
Pathophysiology of ischemic placental disease
Affiliations
- PMID: 24836825
- PMCID: PMC4040272
- DOI: 10.1053/j.semperi.2014.03.005
Item in Clipboard
Review
Pathophysiology of ischemic placental disease
Semin Perinatol.
2014 Apr.
Abstract
The pregnancy disorders associated with placental ischemia share many similar pathological and pathophysiological features and are associated with the failure to deliver adequate nutrients and oxygen to the placenta. The origins of this deficiency are a subject of intense study. In this article, I review the genesis and consequences of this pathology addressing the similarities and the differences with the different disorders and addressing current gaps in our knowledge.
Keywords: intrauterine growth restriction; placenta; placenta ischemia; preeclampsia; premature birth.
Copyright © 2014 Elsevier Inc. All rights reserved.
Figures
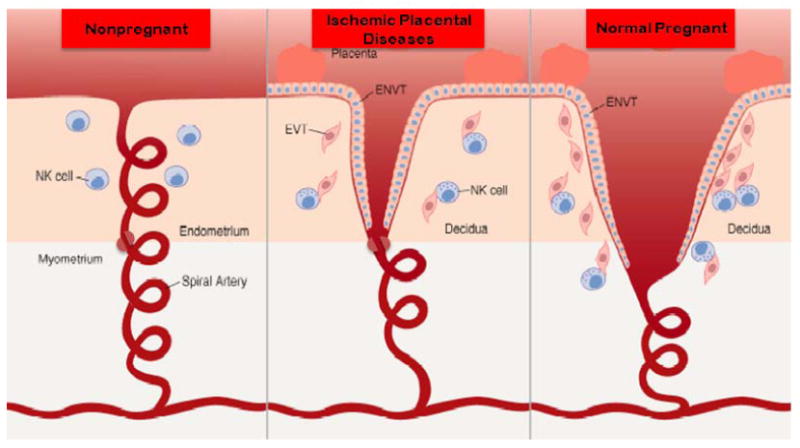
During pregnancy the spiral arteries that underlie the placenta, which in non-pregnant women are typical, small muscular arteries containing smooth muscle and an inner elastic lamina, undergo physiological remodeling. This includes terminal dilatation, the loss of the internal elastic lamina and the loss of smooth muscle. This change extends into the inner third of the myometrium resulting in the loss of a condensation of vascular smooth muscle near the myometrial decidual junction. This “sphincter” is proposed to be responsible for terminating blood flow at the time of menses. In preeclampsia this process is not complete. The terminal dilatation is not as extensive and the removal of smooth muscle is not complete and does not extend beyond the decidua leaving the functional vascular sphincter intact (Reprinted from Parham P. NK cells and trophoblasts: Partners in pregnancy. J Exp Med. 2004; 200(8): 951-5).
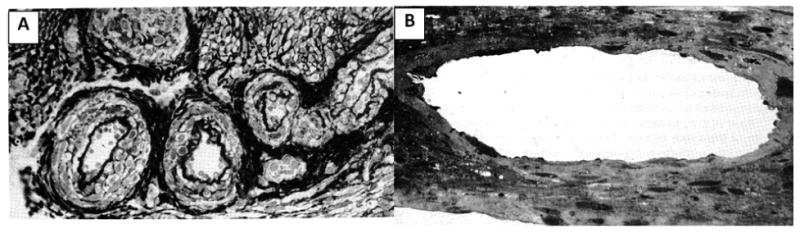
(A) Section of spiral arterioles at the junction of endometrium and myometrium in a nonpregnant individual. Note inner elastic lamina and smooth muscle. (B) Section of spiral arteriole in the same scale and from the same location during pregnancy. Note markedly increased diameter and absence of inner elastic lamina and smooth muscle (Reprinted from Sheppard B, Bonnar J. Uteroplacental arteries and hypertensive pregnancy. In: Bonnar J, MacGillivray I, Symonds G, editors. Pregnancy Hypertension. Baltimore: University Park; 1980. p. 205).
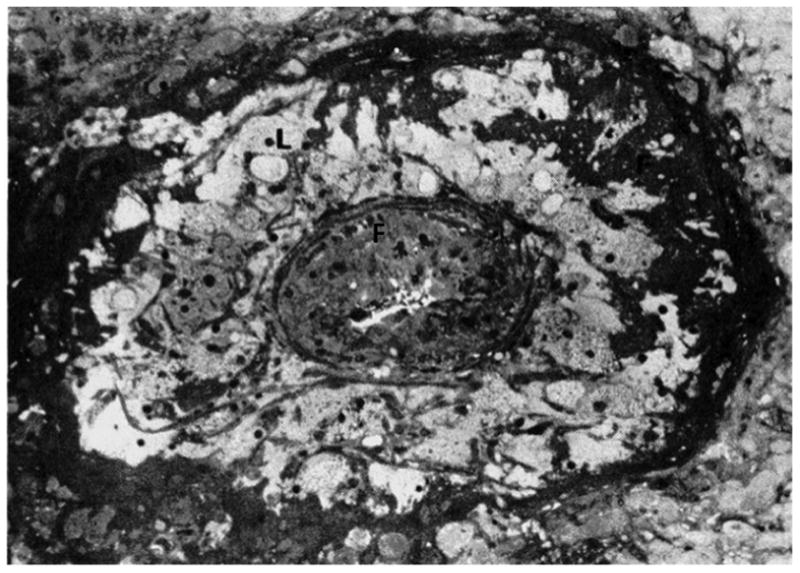
Numerous lipid-laden cells (L) and fibrin deposition (F) are present in the media of this occluded decidual vessel(Reprinted from Sheppard B, Bonnar J. Uteroplacental arteries and hypertensive pregnancy. In: Bonnar J, MacGillivray I, Symonds G, editors. Pregnancy Hypertension. Baltimore: University Park; 1980. p. 205).
References
-
- Burton GJ, Jauniaux E, Charnock-Jones DS. The influence of the intrauterine environment on human placental development. Int J Dev Biol. 2010;54(2-3):303–12. - PubMed
-
- Genbacev O, Zhou Y, Ludlow JW, Fisher SJ. Regulation of human placental development by oxygen tension. Science. 1997;277:1669–72. - PubMed
-
- Pijnenborg R, Vercruysse L, Hanssens A. The uterine spiral arteries in human pregnancy: Facts and controversies. Placenta. 2006;27(9-10):939–58. - PubMed
-
- Brosens I. A study of the spiral arteries of the decidua basalis in normotensive and hypertensive pregnancies. J Obstet Gynaecol Br Commonw. 1964;71:222–30. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
