

National trends in US hospital admissions for hyperglycemia and hypoglycemia among Medicare beneficiaries, 1999 to 2011
- PMID: 24838229
- PMCID: PMC4152370
- DOI: 10.1001/jamainternmed.2014.1824
National trends in US hospital admissions for hyperglycemia and hypoglycemia among Medicare beneficiaries, 1999 to 2011
Abstract
Importance: The increasing intensity of diabetes mellitus management over the past decade may have resulted in lower rates of hyperglycemic emergencies but higher rates of hospital admissions for hypoglycemia among older adults. Trends in these hospitalizations and subsequent outcomes are not known.
Objective: To characterize changes in hyperglycemia and hypoglycemia hospitalization rates and subsequent mortality and readmission rates among older adults in the United States over a 12-year period, and to compare these results according to age, sex, and race.
Design, setting, and patients: Retrospective observational study using data from 33,952,331 Medicare fee-for-service beneficiaries 65 years or older from 1999 to 2011.
Main outcomes and measures: Hospitalization rates for hyperglycemia and hypoglycemia, 30-day and 1-year mortality rates, and 30-day readmission rates.
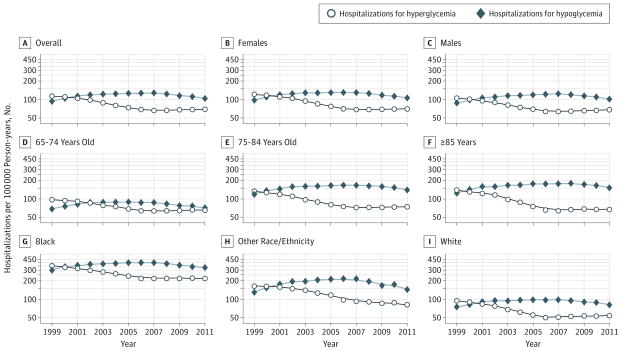
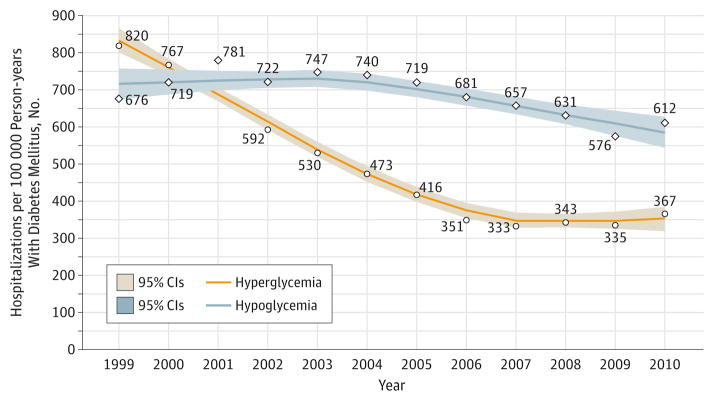
Results: A total of 279,937 patients experienced 302,095 hospitalizations for hyperglycemia, and 404,467 patients experienced 429,850 hospitalizations for hypoglycemia between 1999 and 2011. During this time, rates of admissions for hyperglycemia declined by 38.6% (from 114 to 70 admissions per 100,000 person-years), while admissions for hypoglycemia increased by 11.7% (from 94 to 105 admissions per 100,000 person-years). In analyses designed to account for changing diabetes mellitus prevalence, admissions for hyperglycemia and hypoglycemia declined by 55.2% and 9.5%, respectively. Trends were similar across age, sex, and racial subgroups, but hypoglycemia rates were 2-fold higher for older patients (≥75 years) when compared with younger patients (65-74 years), and admission rates for both hyperglycemia and hypoglycemia were 4-fold higher for black patients compared with white patients. The 30-day and 1-year mortality and 30-day readmission rates improved during the study period and were similar after an index hospitalization for either hyperglycemia or hypoglycemia (5.4%, 17.1%, and 15.3%, respectively, after hyperglycemia hospitalizations in 2010; 4.4%, 19.9%, and 16.3% after hypoglycemia hospitalizations).
Conclusions and relevance: Hospital admission rates for hypoglycemia now exceed those for hyperglycemia among older adults. Although admissions for hypoglycemia have declined modestly since 2007, rates among black Medicare beneficiaries and those older than 75 years remain high. Hospital admissions for severe hypoglycemia seem to pose a greater health threat than those for hyperglycemia, suggesting new opportunities for improvement in care of persons with diabetes mellitus.
Conflict of interest statement
Figures
Comment in
-
Hospital admissions for hypoglycemia now exceed those for hyperglycemia in Medicare beneficiaries.JAMA Intern Med. 2014 Jul;174(7):1125. doi: 10.1001/jamainternmed.2014.2192. JAMA Intern Med. 2014. PMID: 24838084 No abstract available.
References
-
- Johnston SS, Conner C, Aagren M, Ruiz K, Bouchard J. Association between hypoglycaemic events and fall-related fractures in Medicare-covered patients with type 2 diabetes. Diabetes Obes Metab. 2012;14(7):634–643. - PubMed
-
- Zoungas S, Patel A, Chalmers J, et al. ADVANCE Collaborative Group. Severe hypoglycemia and risks of vascular events and death. N Engl J Med. 2010;363(15):1410–1418. - PubMed
Publication types
MeSH terms
Grants and funding
- K08 AG032886-05/AG/NIA NIH HHS/United States
- T32AG1934/AG/NIA NIH HHS/United States
- R03 AG045086/AG/NIA NIH HHS/United States
- P30 AG021342/AG/NIA NIH HHS/United States
- U01 HL105270/HL/NHLBI NIH HHS/United States
- T32 DK097718/DK/NIDDK NIH HHS/United States
- K23 AG048359/AG/NIA NIH HHS/United States
- R01 DK065664/DK/NIDDK NIH HHS/United States
- UL1 TR000142/TR/NCATS NIH HHS/United States
- L30 AG045923/AG/NIA NIH HHS/United States
- K08 AG032886/AG/NIA NIH HHS/United States
- P30 DK092949/DK/NIDDK NIH HHS/United States
- R01 DK081796/DK/NIDDK NIH HHS/United States
- K07AG043587/AG/NIA NIH HHS/United States
- K07 AG043587/AG/NIA NIH HHS/United States
- R01 DK65664/DK/NIDDK NIH HHS/United States
- P30 AG21342/AG/NIA NIH HHS/United States
- P30 DK092924/DK/NIDDK NIH HHS/United States
- T32DK097718/DK/NIDDK NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
