

Axonal loss of retinal neurons in multiple sclerosis associated with optic radiation lesions
- PMID: 24838786
- PMCID: PMC4113462
- DOI: 10.1212/WNL.0000000000000522
Axonal loss of retinal neurons in multiple sclerosis associated with optic radiation lesions
Abstract
Objective: To investigate the potential links between thinning of retinal ganglion cell axons in eyes of patients with multiple sclerosis (MS) without past optic neuritis (ON) and MS-related inflammatory damage of the posterior visual pathway.
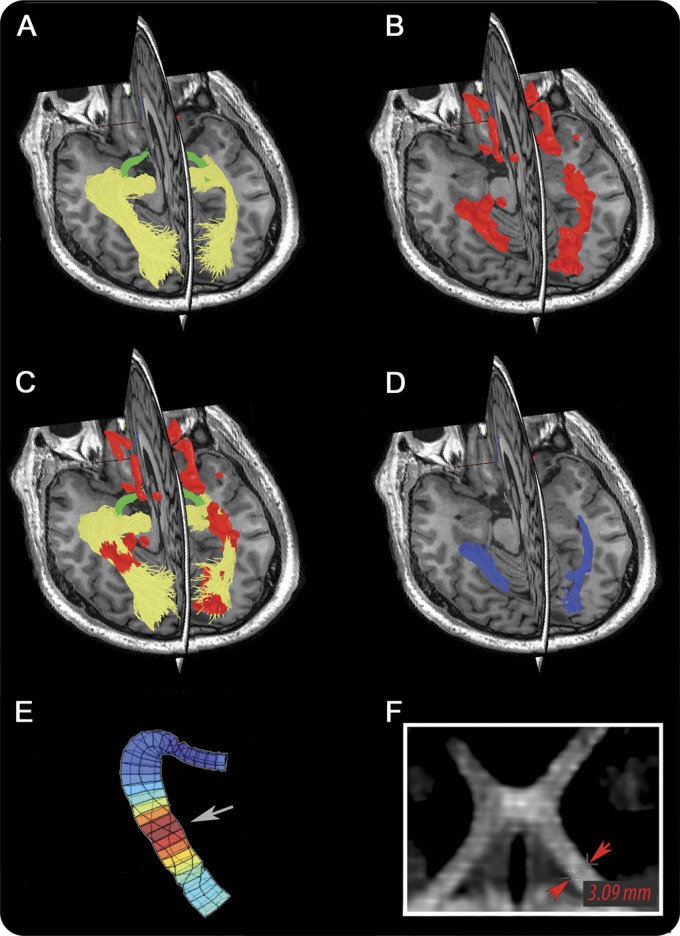
Methods: Temporal retinal nerve fiber layer (tRNFL) thickness was analyzed in eyes with no history of ON (NON) from 53 patients with relapsing-remitting MS. Fifty normal age- and sex-matched controls were examined with optical coherence tomography. Low-contrast visual acuity charts were used for functional assessment of vision. The optic tract (OT) and optic radiation (OR) were identified using probabilistic tractography, and volume of T2 fluid-attenuated inversion recovery lesions and diffusion tensor imaging (DTI) indices were measured within both structures. Cross-sectional diameter of the OT was also calculated.
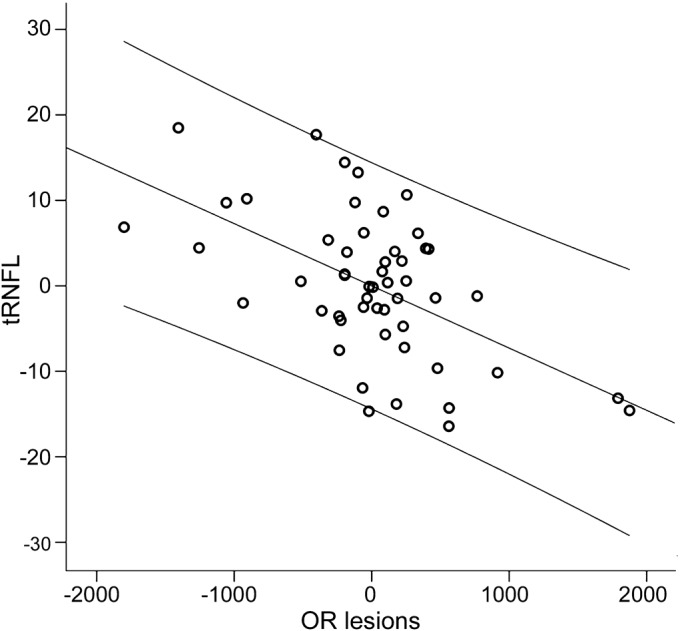
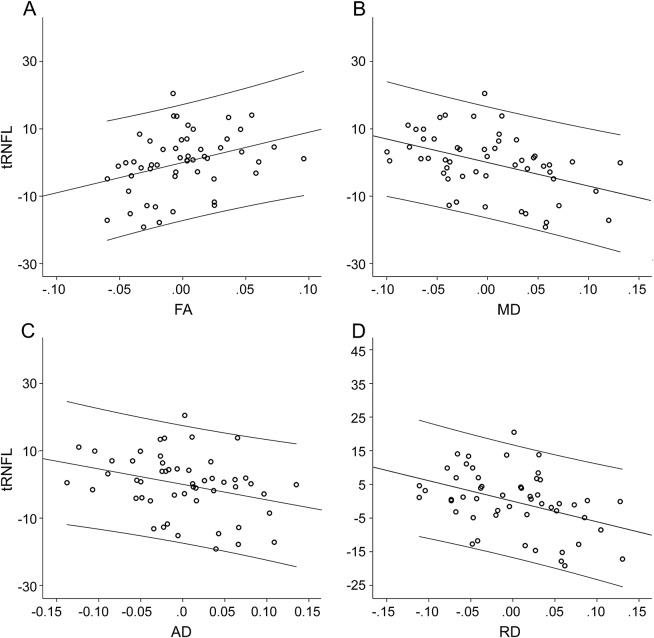
Results: tRNFL thickness was significantly reduced in NON eyes and was associated with reduced low-contrast visual acuity. Lesions within the OR were detected in the majority of patients. There was a significant correlation between thinning of the tRNFL and OR lesion volume (adjusted for non-OR lesion volume, age, sex, and disease duration). tRNFL thickness also correlated with OR DTI indices. No OT lesions were identified in any of the patients and no relationship between retinal nerve fiber layer loss and potential markers of OT lesions was found.
Conclusion: The results demonstrate a strong tract-specific association between loss of tRNFL fibers and MS-related inflammation within OR.
© 2014 American Academy of Neurology.
Figures
Comment in
-
Retrograde trans-synaptic degeneration in MS: a missing link?Neurology. 2014 Jun 17;82(24):2152-3. doi: 10.1212/WNL.0000000000000532. Epub 2014 May 16. Neurology. 2014. PMID: 24838792 No abstract available.
References
-
- Sorensen TL, Frederiksen JL, Bronnum-Hansen H, Petersen HC. Optic neuritis as onset manifestation of multiple sclerosis. Neurology 1999;53:473–478 - PubMed
-
- Hornabrook RS, Miller D, Newton MR, et al. Frequent involvement of optic radiation in patients with acute isolated optic neuritis. Neurology 1992;42:77–79 - PubMed
-
- Petzold A, de Boer JF, Schippling S, et al. Optical coherence tomography in multiple sclerosis: a systematic review and meta-analysis. Lancet Neurol 2010;9:921–932 - PubMed
-
- Klistorner A, Garrick R, Barnett MH, et al. Axonal loss in non-optic neuritis eyes of patients with multiple sclerosis linked to delayed visual evoked potential. Neurology 2013;15:242–245 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous