

Accuracy and reproducibility of automated, standardized coronary transluminal attenuation gradient measurements
- PMID: 24839136
- PMCID: PMC4104747
- DOI: 10.1007/s10554-014-0446-4
Accuracy and reproducibility of automated, standardized coronary transluminal attenuation gradient measurements
Abstract
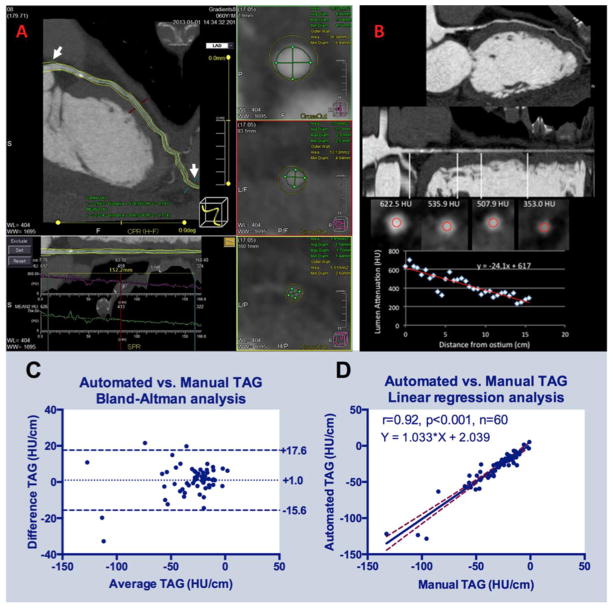
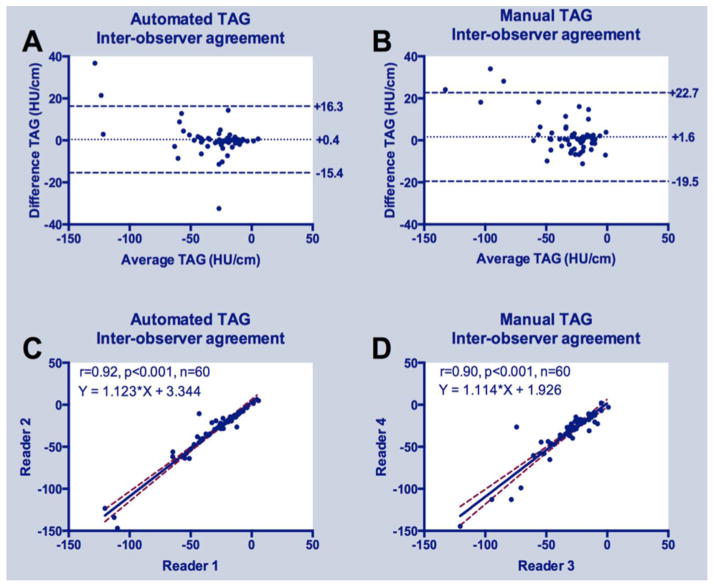
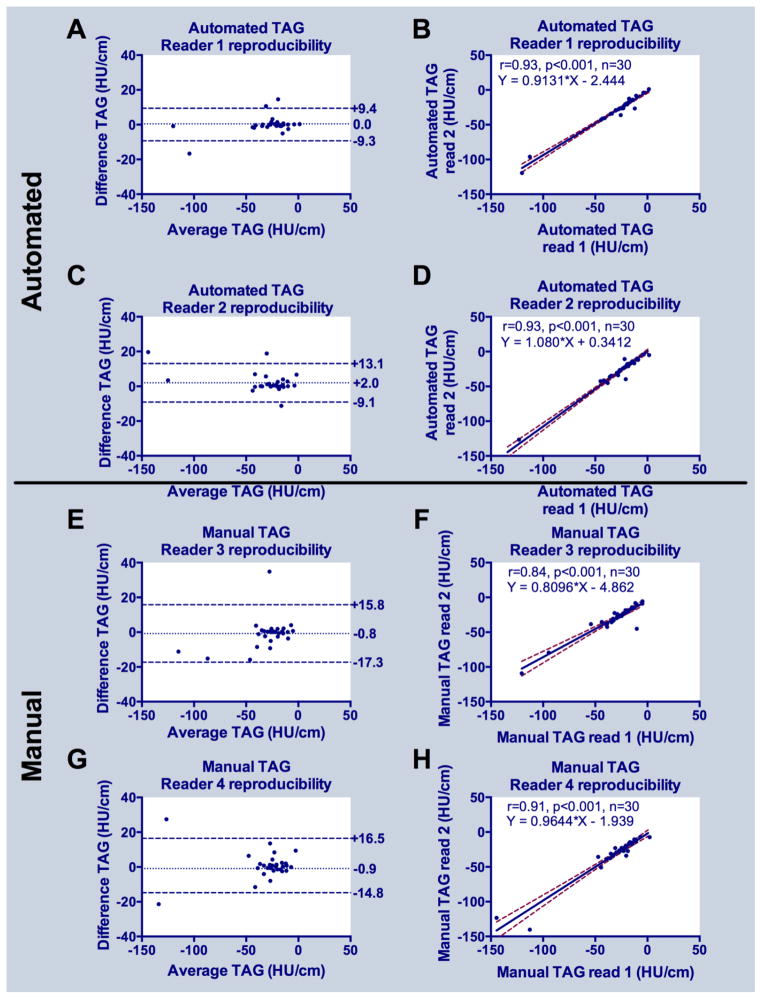
Coronary computed tomography angiography (CCTA) contrast opacification gradients, or transluminal attenuation gradients (TAG) offer incremental value to predict functionally significant lesions. This study introduces and evaluates an automated gradients software package that can potentially supplant current, labor-intensive manual TAG calculation methods. All 60 major coronary arteries in 20 patients who underwent a clinically indicated single heart beat 320 × 0.5 mm detector row CCTA were retrospectively evaluated by two readers using a previously validated manual measurement approach and two additional readers who used the new automated gradient software. Accuracy of the automated method against the manual measurements, considered the reference standard, was assessed via linear regression and Bland-Altman analyses. Inter- and intra-observer reproducibility and factors that can affect accuracy or reproducibility of both manual and automated TAG measurements, including CAD severity and iterative reconstruction, were also assessed. Analysis time was reduced by 68% when compared to manual TAG measurement. There was excellent correlation between automated TAG and the reference standard manual TAG. Bland-Altman analyses indicated low mean differences (1 HU/cm) and narrower inter- and intra-observer limits of agreement for automated compared to manual measurements (25 and 36% reduction with automated software, respectively). Among patient and technical factors assessed, none affected agreement of manual and automated TAG measurement. Automated 320 × 0.5 mm detector row gradient software reduces computation time by 68% with high accuracy and reproducibility.
Conflict of interest statement
Figures
References
-
- Levine GN, Bates ER, Blankenship JC, et al. 2011 ACCF/AHA/SCAI Guideline for Percutaneous Coronary Intervention: executive summary: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Catheter Cardiovasc Interv. 2012;79(3):453–95. - PubMed
-
- Tonino PA, De Bruyne B, Pijls NH, et al. Fractional flow reserve versus angiography for guiding percutaneous coronary intervention. N Engl J Med. 2009;360(3):213–24. - PubMed
-
- Choi JH, Min JK, Labounty TM, et al. Intracoronary transluminal attenuation gradient in coronary CT angiography for determining coronary artery stenosis. JACC Cardiovasc Imaging. 2011;4(11):1149–57. - PubMed
-
- Chow BJ, Kass M, Gagne O, et al. Can differences in corrected coronary opacification measured with computed tomography predict resting coronary artery flow? J Am Coll Cardiol. 2011;57(11):1280–8. - PubMed
-
- Lackner K, Bovenschulte H, Stutzer H, Just T, Al-Hassani H, Krug B. In vitro measurements of flow using multislice computed tomography (MSCT) Int J Cardiovasc Imaging. 2010 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
