

Current and emerging treatments and surgical interventions for Morquio A syndrome: a review
- PMID: 24839594
- PMCID: PMC4020877
- DOI: 10.2147/RRED.S37278
Current and emerging treatments and surgical interventions for Morquio A syndrome: a review
Abstract
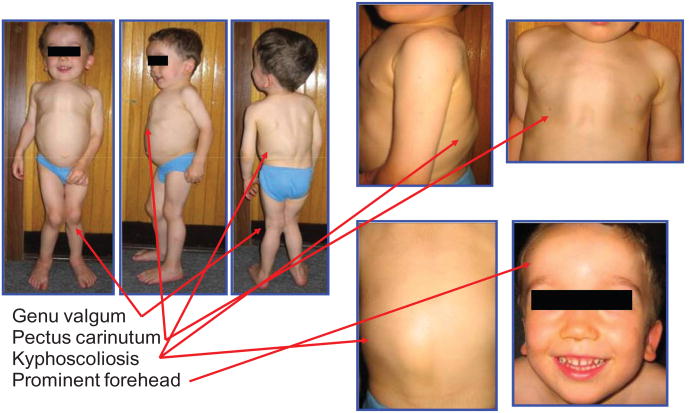
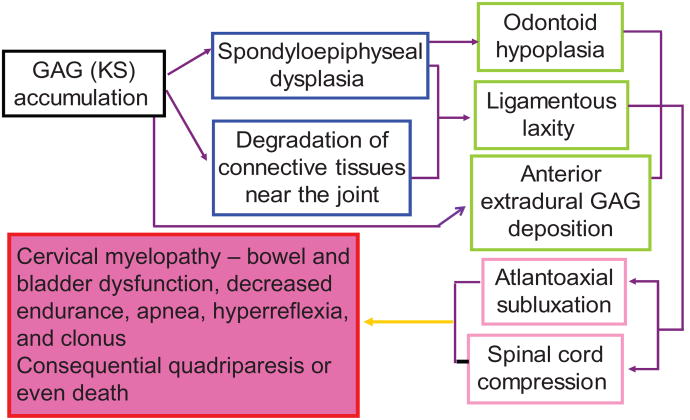
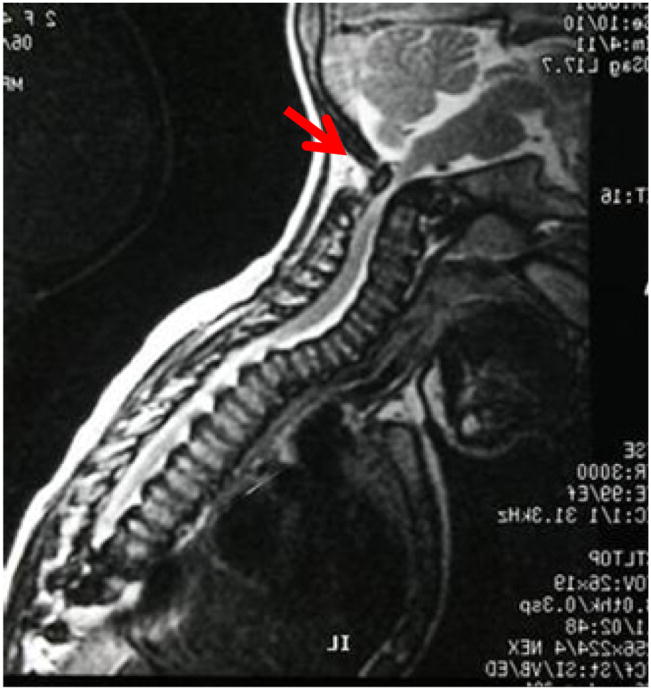
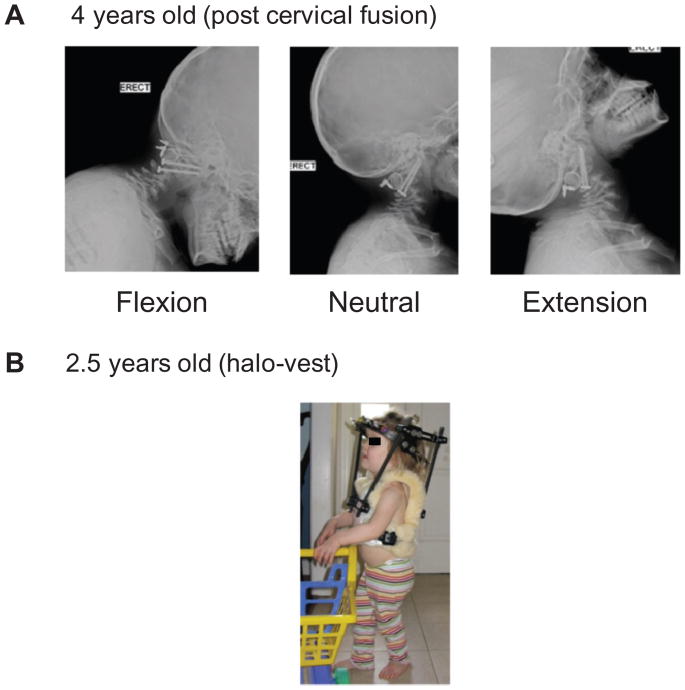
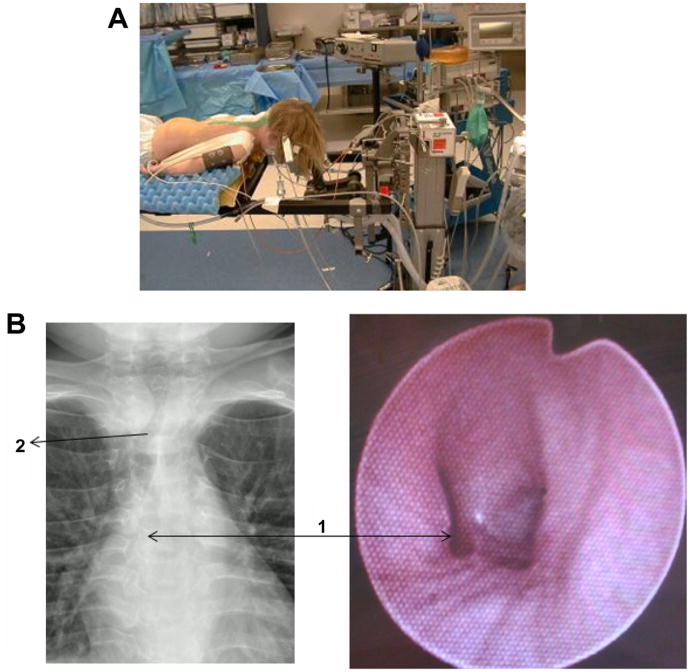
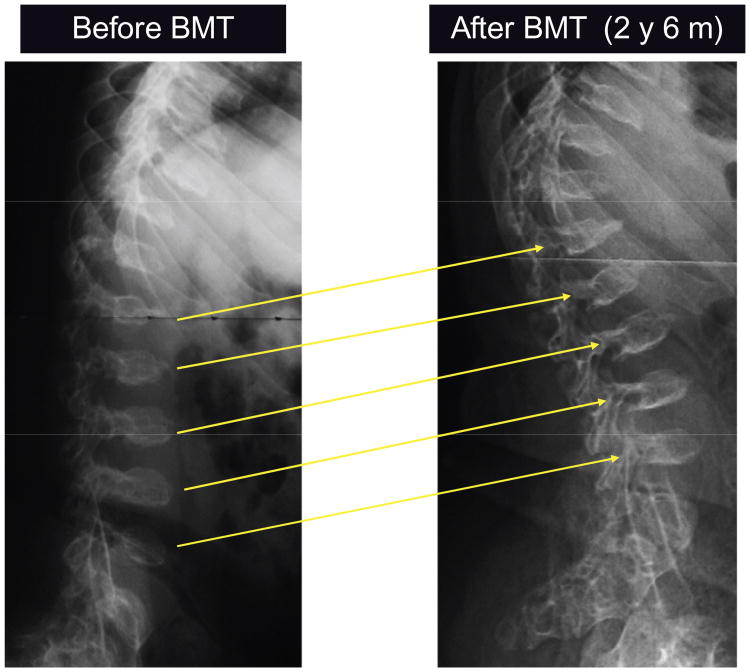
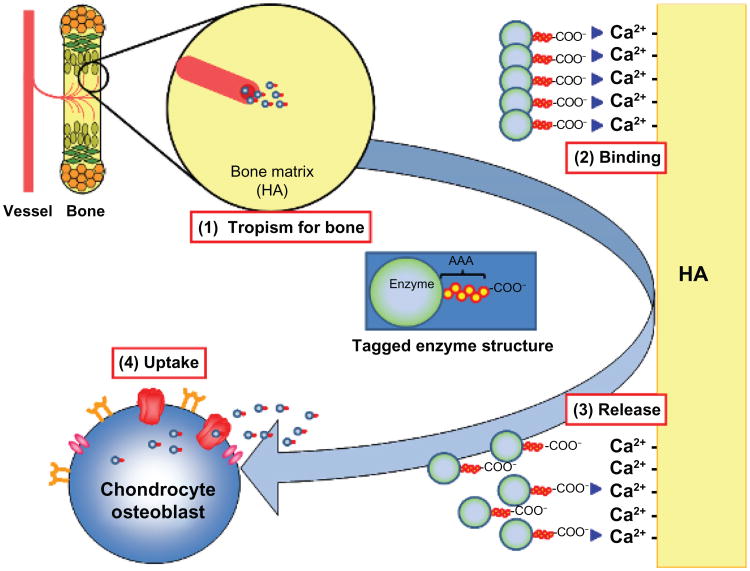
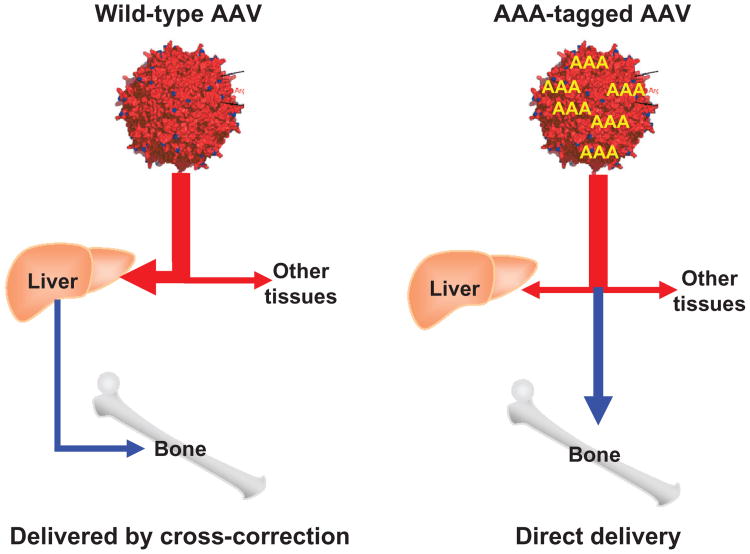
Patients with mucopolysaccharidosis type IVA (MPS IVA; Morquio A syndrome) have accumulation of the glycosaminoglycans, keratan sulfate, and chondroitin-6-sulfate, in bone and cartilage, causing systemic spondyloepiphyseal dysplasia. Features include lumbar gibbus, pectus carinatum, faring of the rib cage, marked short stature, cervical instability and stenosis, kyphoscoliosis, genu valgum, and laxity of joints. Generally, MPS IVA patients are wheelchair-bound as teenagers and do not survive beyond the second or third decade of life as a result of severe bone dysplasia, causing restrictive lung disease and airway narrowing, increasing potential for pneumonia and apnea; stenosis and instability of the upper cervical region; high risk during anesthesia administration due to narrowed airway as well as thoracoabdominal dysfunction; and surgical complications. Patients often need multiple surgical procedures, including cervical decompression and fusion, hip reconstruction and replacement, and femoral or tibial osteotomy, throughout their lifetime. Current measures to intervene in disease progression are largely palliative, and improved therapies are urgently needed. A clinical trial for enzyme replacement therapy (ERT) and an investigational trial for hematopoietic stem cell transplantation (HSCT) are underway. Whether sufficient enzyme will be delivered effectively to bone, especially cartilage (avascular region) to prevent the devastating skeletal dysplasias remains unclear. This review provides an overview of historical aspects of studies on MPS IVA, including clinical manifestations and pathogenesis of MPS IVA, orthopedic surgical interventions, and anesthetic care. It also describes perspectives on potential ERT, HSCT, and gene therapy.
Keywords: GALNS; enzyme replacement therapy; gene therapy; hematopoietic stem cell transplantation; keratan sulfate; mucopolysaccharidosis IVA.
Conflict of interest statement
Figures
References
-
- Meikle PJ, Hopwood JJ, Clague AE, Carey WF. Prevalence of lysosomal storage disorders. JAMA. 1999;281(3):249–254. - PubMed
-
- Applegarth DA, Toone JR, Lowry RB. Incidence of inborn errors of metabolism in British Columbia, 1969–1996. Pediatrics. 2000;105(1):e10. - PubMed
-
- Nelson J. Incidence of the mucopolysaccharidoses in Northern Ireland. Hum Genet. 1997;101(3):355–358. - PubMed
-
- Poorthuis BJ, Wevers RA, Kleijer WJ, et al. The frequency of lysosomal storage diseases in The Netherlands. Hum Genet. 1999;105(1–2):151–156. - PubMed
-
- Pinto R, Caseiro C, Lemos M, et al. Prevalence of lysosomal storage diseases in Portugal. Eur J Hum Genet. 2004;12(2):87–92. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources