

Burden of disease and cost of chronic hepatitis C infection in Canada
- PMID: 24839620
- PMCID: PMC4049256
- DOI: 10.1155/2014/317623
Burden of disease and cost of chronic hepatitis C infection in Canada
Abstract
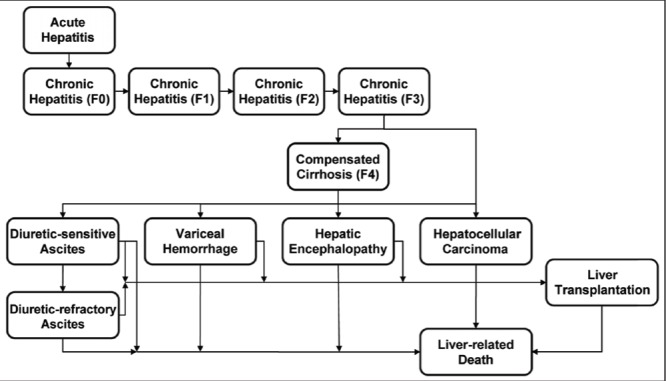
Background: Chronic infection with hepatitis C virus (HCV) is a major cause of cirrhosis, hepatocellular carcinoma and liver transplantation.
Objective: To estimate the burden of HCV-related disease and costs from a Canadian perspective.
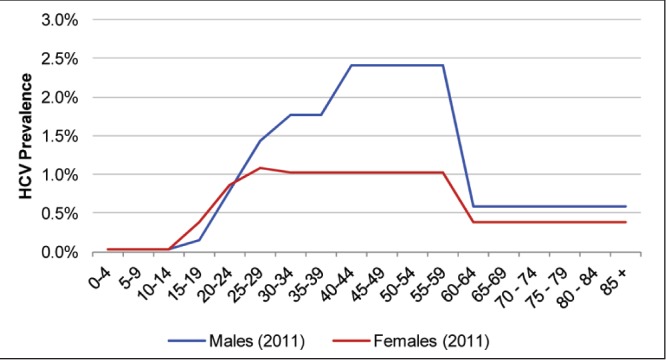
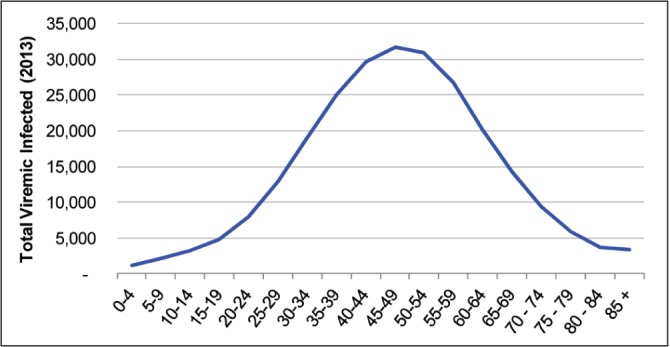
Methods: Using a system dynamic framework, the authors quantified the HCV-infected population, disease progression and costs in Canada between 1950 and 2035. Specifically, 36 hypothetical, age- and sex-defined cohorts were tracked to define HCV prevalence, complications and direct medical costs (excluding the cost of antivirals). Model assumptions and costs were extracted from the literature with an emphasis on Canadian data. No incremental increase in antiviral treatment over current levels was assumed, despite the future availability of potent antivirals.
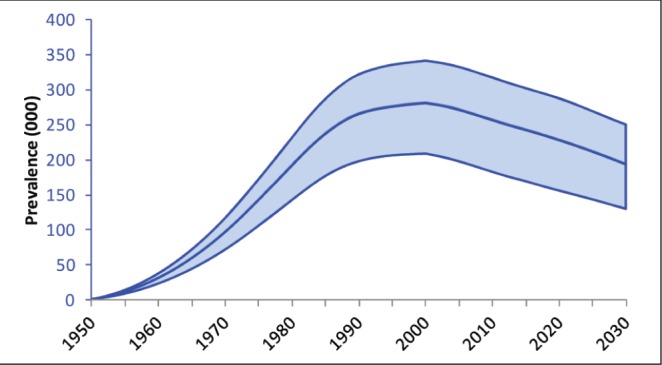
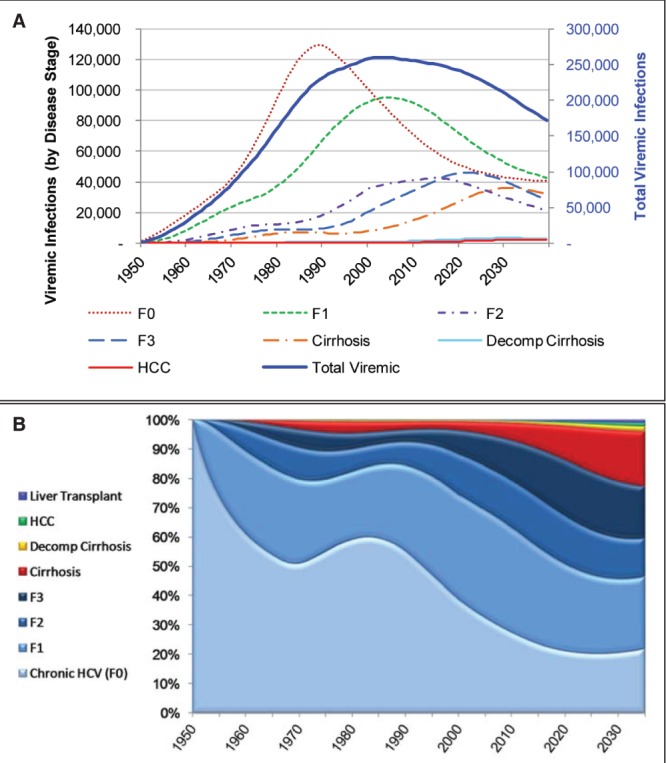
Results: The estimated prevalence of viremic hepatitis C cases peaked in 2003 at 260,000 individuals (uncertainty interval 192,460 to 319,880), reached 251,990 (uncertainty interval 177,890 to 314,800) by 2013 and is expected to decline to 188,190 (uncertainty interval 124,330 to 247,200) in 2035. However, the prevalence of advanced liver disease is increasing. The peak annual number of patients with compensated cirrhosis (n=36,210), decompensated cirrhosis (n=3380), hepatocellular carcinoma (n=2220) and liver-related deaths (n=1880) are expected to occur between 2031 and 2035. During this interval, an estimated 32,460 HCV-infected individuals will die of liver-related causes. Total health care costs associated with HCV (excluding treatment) are expected to increase by 60% from 2013 until the peak in 2032, with the majority attributable to cirrhosis and its complications (81% in 2032 versus 56% in 2013). The lifetime cost for an individual with HCV infection in 2013 was estimated to be $64,694.
Conclusions: Although the prevalence of HCV in Canada is decreasing, cases of advanced liver disease and health care costs continue to rise. These results will facilitate disease forecasting, resource planning and the development of rational management strategies for HCV in Canada.
HISTORIQUE :: L’infection chronique par le virus de l’hépatite C (VHC) est une cause importante de cirrhose, de carcinome hépatocellulaire et de transplantation hépatique.
OBJECTIF :: Évaluer le fardeau et le coût des maladies liées au VIH dans une perspective canadienne.
MÉTHODOLOGIE :: Dans un cadre dynamique, les auteurs ont quantifié la population infectée par le VHC, ainsi que l’évolution et le coût de la maladie au Canada entre 1950 et 2035. Plus précisément, 36 cohortes hypothétiques, définies en fonction de l’âge et du sexe, ont été suivies pour définir la prévalence, les complications et les coûts médicaux directs (à l’exception du coût des antiviraux) du VHC. Les hypothèses et les coûts des modèles ont été tirés des publications, particulièrement celles d’origine canadienne. Aucune augmentation incrémentielle du traitement aux antiviraux n’a été présumée par rapport aux taux actuels, malgré l’accessibilité potentielle à de futurs antiviraux.
RÉSULTATS :: La prévalence estimative des cas d’hépatite C virémique a atteint un sommet en 2003, avec 260 000 individus (intervalle d’incertitude de 192 460 à 319 880). Elle a atteint 251 990 (intervalle d’incertitude de 177 890 à 314 800) en 2013 et devrait reculer à 188 190 (intervalle d’incertitude de 124 330 à 247 200) en 2035. Cependant, la prévalence de maladie hépatique avancée augmente. Le nombre annuel maximal de patients ayant une cirrhose compensée (n=36 210), une cirrhose décompensée (n=3 380), un carcinome hépatocellulaire (n=2 220) et décédés à cause de problèmes hépatiques (n=1 880) devrait être atteint entre 2031 et 2035. Pendant cet intervalle, on estime que 32 460 personnes infectées par le VHC mourront d’une cause liée à un problème hépatique. Les coûts de santé totaux associés au VHC (à l’exclusion du traitement) devraient augmenter de 60 % entre 2013 et le sommet de 2032, en majorité à cause de la cirrhose et de ses complications (81 % en 2032, par rapport à 56 % en 2013). En 2013, le coût à vie d’une personne atteinte d’une infection par le VHC était évalué à 64 694 $.
CONCLUSIONS :: Même si la prévalence de VHC diminue au Canada, les cas de maladie hépatique avancée et les coûts des soins continuent d’augmenter. Ces résultats contribueront à la prévision des maladies, à la planification des ressources et à l’élaboration de stratégies rationnelles de prise en charge du VHC au Canada.
Figures
References
-
- Mohd Hanafiah K, Groeger J, Flaxman AD, Wiersma ST. Global epidemiology of hepatitis C virus infection: New estimates of age-specific antibody to HCV seroprevalence. Hepatology. 2013;57:1333–42. - PubMed
-
- Trubnikov M. Developing estimates of prevalent and undiagnosed HCV infection in Canada in 2011. < www.youtube.com/watch?v=234ru9AFA6U&list=PLy0zwf7_pKrXSh9bx6XxznPv65S44n...> (Accessed February 9, 2014)
-
- Remis RS. Modelling the incidence and prevalence of hepatitis C infection and its sequelae in Canada, 2007: Final report. Community Acquired Infections Division, Centre for Communicable Diseases and Infection Control, Public Health Agency of Canada; 2009. < http://epe.lac-bac.gc.ca/100/200/301/phac-aspc/modeling_hepatis_c_infect...> (Accessed February 9, 2014)
-
- Canadian Liver Foundation. Liver disease in Canada – a crisis in the making. < www.liverca/support-liver-foundation/advocate/Liver_Disease_in_Canada_Re...> (Accessed February 9, 2014)
-
- Zou S, Tepper M, El Saadany S. Prediction of hepatitis C burden in Canada. Can J Gastroenterol. 2000;14:575–80. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
