

A randomized trial of edivoxetine in pediatric patients with attention-deficit/hyperactivity disorder
- PMID: 24840045
- PMCID: PMC4026219
- DOI: 10.1089/cap.2013.0043
A randomized trial of edivoxetine in pediatric patients with attention-deficit/hyperactivity disorder
Abstract
Objective: The purpose of this study was to assess the efficacy and safety of edivoxetine (LY2216684), a selective norepinephrine reuptake inhibitor, in pediatric patients with attention-deficit/hyperactivity disorder (ADHD).
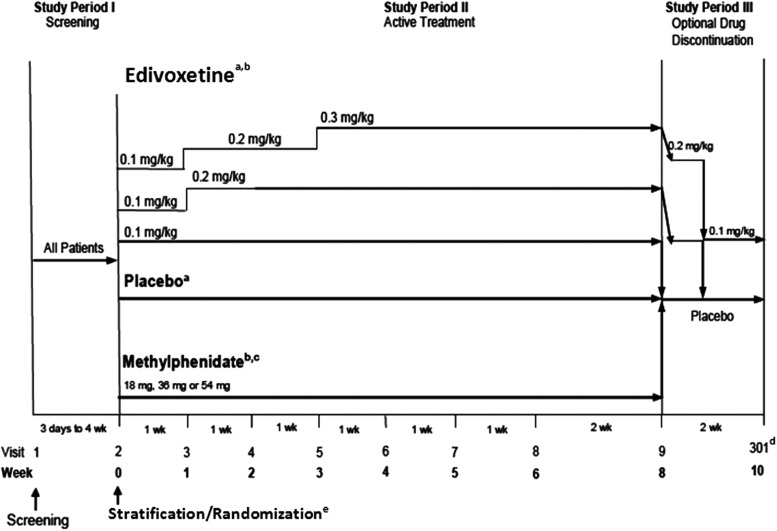
Method: A fixed-dose, randomized, double-blind, 8 week study was conducted in patients 6-17 years of age, who were randomized by two strata: 1) Patients with prior stimulant use randomized to placebo, edivoxetine 0.1 mg/kg/day, 0.2 mg/kg/day, or 0.3 mg/kg/day arms in a 1:1:1:1 ratio; 2) Stimulant-naïve patients randomized to placebo, edivoxetine 0.1mg/kg/day, 0.2 mg/kg/day, 0.3 mg/kg/day, or osmotic-release oral system methylphenidate (OROS MPH) (18-54 mg/day based on body weight) arms in a 1:1:1:1:1 ratio. The primary efficacy measure was baseline-to-week 8 change of ADHD Rating Scale (ADHD-RS) total score for edivoxetine 0.2 mg/kg/day and 0.3 mg/kg/day.
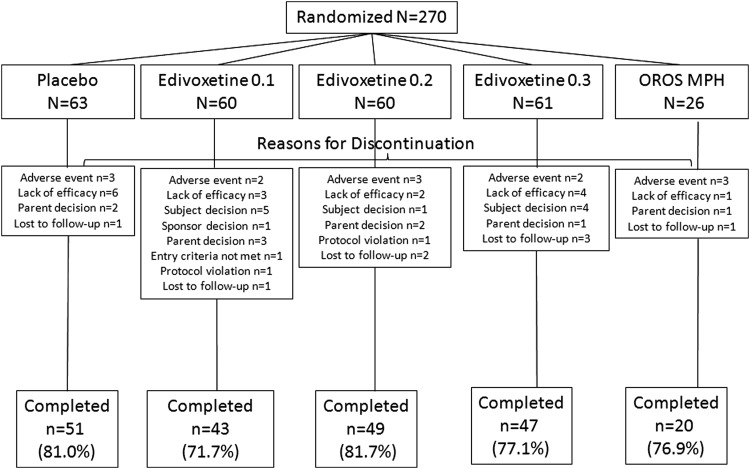
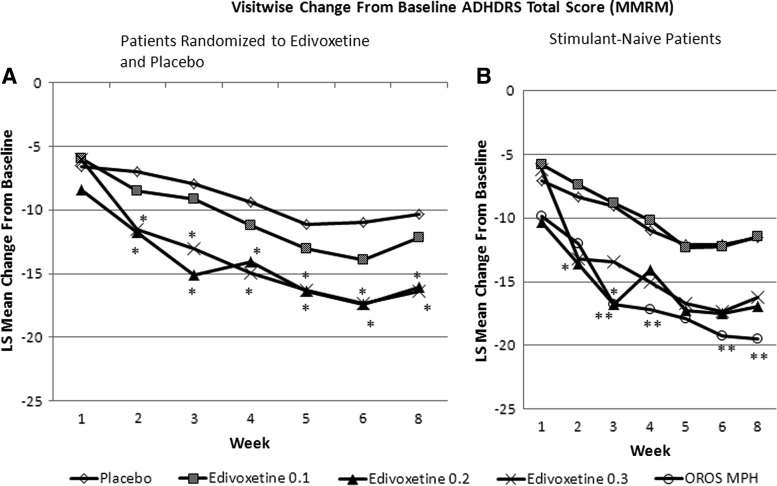
Results: A total of 340 patients were randomized to placebo (n=78); edivoxetine 0.1 mg/kg/day (n=76), 0.2 mg/kg/day (n=75), or 0.3 mg/kg/day (n=75); or OROS MPH (n=36). In the stimulant-naïve stratum, the positive control, OROS MPH, was significantly superior to placebo in mean ADHD-RS total score change at end-point (-19.46, p=0.015). The edivoxetine 0.2 mg/kg/day and 0.3 mg/kg/day arms had statistically significantly greater improvement than the placebo arm in mean ADHD-RS total score change at end-point (placebo -10.35; edivoxetine 0.2 mg/kg/day -16.09, p<0.010; edivoxetine 0.3 mg/kg/day -16.39, p<0.010) and Clinical Global Impressions-Improvement score (placebo 3.05; edivoxetine 0.1 mg/kg/day 3.01, p=0.860; edivoxetine 0.2 mg/kg/day 2.54, p=0.013; edivoxetine 0.3 mg/kg/day 2.53, p=0.013). In the overall efficacy-analyses data set (n=270), the effect size estimates for edivoxetine doses 0.1 mg/kg/day, 0.2 mg/kg/day and 0.3 mg/kg/day at the week 8 time point were 0.17, 0.51, and 0.54, respectively (for the stimulant-naïve stratum, the effect size estimate for OROS MPH was 0.69). Compared with placebo, edivoxetine treatment was associated with statistically significant increases in blood pressure and pulse (p<0.050), and a smaller increase or slight decrease in weight.
Conclusions: Edivoxetine at doses of 0.2 mg/kg/day and 0.3 mg/kg/day demonstrated efficacy in ADHD treatment, despite the presence of a sizeable placebo response. No unexpected adverse events were identified. Clinical Trial Registry identifier: NCT00922636.
Figures
References
-
- American Psychiatric Association: Diagnostic and Statistical Manual of Mental Disorders, 4th ed., Text Revision. Washington, DC: American Psychiatric Association; 2000
-
- Conners CK: Conners Rating Scales - Revised. North Tonawanda, New York: Multi-Health Systems, Inc.; 1997
-
- Culpepper L: Primary care treatment of attention-deficit/hyperactivity disorder. J Clin Psychiatry 67Suppl 8:51–58, 2006 - PubMed
-
- Del Campo N, Chamberlain SR, Sahakian BJ, Robbins TW: The roles of dopamine and noradrenaline in the pathophysiology and treatment of attention-deficit/hyperactivity disorder. Biol Psychiatry 69:e145–e157, 2011 - PubMed
-
- DuPaul GJ, Power TJ, Anastopoulos AD, Reid R: ADHD Rating Scale-IV: Checklists, norms, and clinical interpretations. New York, Guilford Press, 1998
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
