

The glomerulopathy of sickle cell disease
- PMID: 24840607
- PMCID: PMC4320776
- DOI: 10.1002/ajh.23762
The glomerulopathy of sickle cell disease
Abstract
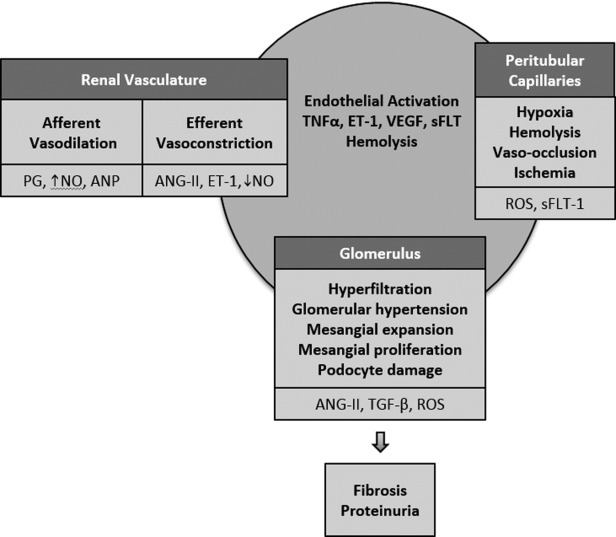
Sickle cell disease (SCD) produces many structural and functional abnormalities in the kidney, including glomerular abnormalities. Albuminuria is the most common manifestation of glomerular damage, with a prevalence between 26 and 68% in adult patients. The pathophysiology of albuminuria in SCD is likely multifactorial, with contributions from hyperfiltration, glomerular hypertension, ischemia-reperfusion injury, oxidative stress, decreased nitric oxide (NO) bioavailability, and endothelial dysfunction. Although its natural history in SCD remains inadequately defined, albuminuria is associated with increased echocardiography-derived tricuspid regurgitant jet velocity, systemic blood pressure, and hypertension, as well as history of stroke, suggesting a shared vasculopathic pathophysiology. While most patients with albuminuria are treated with angiotensin converting enzyme inhibitors/angiotensin receptor blockers, there are no published long-term data on the efficacy of these agents. With the improved patient survival following kidney transplantation, SCD patients with end-stage renal disease should be considered for this treatment modality. Given the high prevalence of albuminuria and its association with multiple SCD-related clinical complications, additional studies are needed to answer several clinically important questions in a bid to adequately elucidate its pathophysiology, natural history, and treatment.
© 2014 The Authors American Journal of Hematology Published by Wiley Periodicals, Inc.
Figures
References
-
- Ataga KI, Orringer EP. Renal abnormalities in sickle cell disease. Am J Hematol. 2000;63:205–211. - PubMed
-
- Falk RJ, Jenette JC. Renal disease. In: Embury SH, Hebbel RP, Mohandas N, Steinberg MH, editors. Sickle Cell Disease: Basic Principles and Clinical Practice. New York: Raven Press; 1994. pp. 673–680.
-
- Sears DA. The morbidity of sickle cell trait: A review of the literature. Am J Med. 1978;64:1021–1036. - PubMed
-
- Kiryluk K, Jadoon A, Gupta M, Radhakrishnan J. Sickle cell trait and gross hematuria. Kidney Int. 2007;71:706–710. - PubMed
-
- Statius van Eps LW, Pinedo-Veels C, de Vries CH. Nature of concentrating defect in sickle cell nephropathy, microangiographic studies. Lancet. 1970;1:450–452. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical