

Cost-effectiveness of the children's oncology group long-term follow-up screening guidelines for childhood cancer survivors at risk for treatment-related heart failure
- PMID: 24842414
- PMCID: PMC4073480
- DOI: 10.7326/M13-2498
Cost-effectiveness of the children's oncology group long-term follow-up screening guidelines for childhood cancer survivors at risk for treatment-related heart failure
Abstract
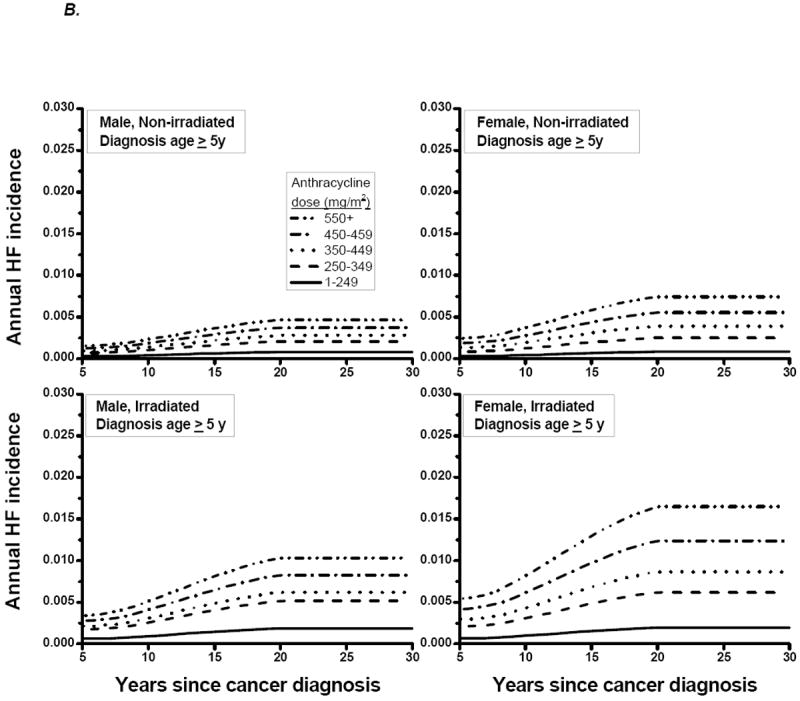
Background: Childhood cancer survivors treated with anthracyclines are at high risk for asymptomatic left ventricular dysfunction (ALVD), subsequent heart failure, and death. The consensus-based Children's Oncology Group (COG) Long-Term Follow-up Guidelines recommend lifetime echocardiographic screening for ALVD.
Objective: To evaluate the efficacy and cost-effectiveness of the COG guidelines and to identify more cost-effective screening strategies.
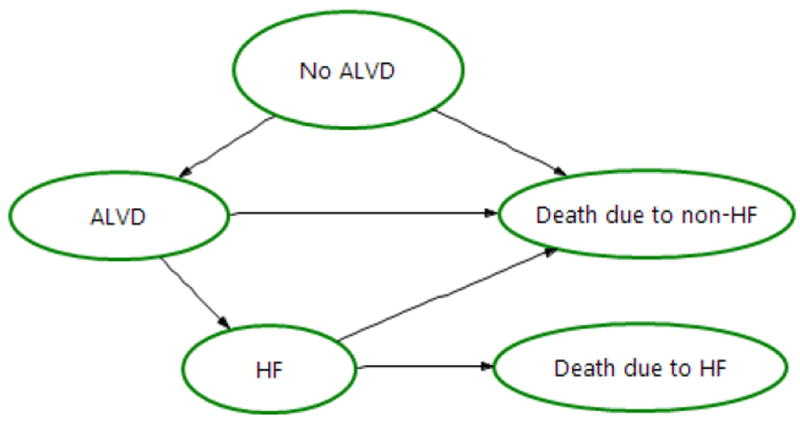
Design: Simulation of life histories using Markov health states.
Data sources: Childhood Cancer Survivor Study; published literature.
Target population: Childhood cancer survivors.
Time horizon: Lifetime.
Perspective: Societal.
Intervention: Echocardiographic screening followed by angiotensin-converting enzyme (ACE) inhibitor and β-blocker therapies after ALVD diagnosis.
Outcome measures: Quality-adjusted life-years (QALYs), costs, incremental cost-effectiveness ratios (ICERs) in dollars per QALY, and cumulative incidence of heart failure.
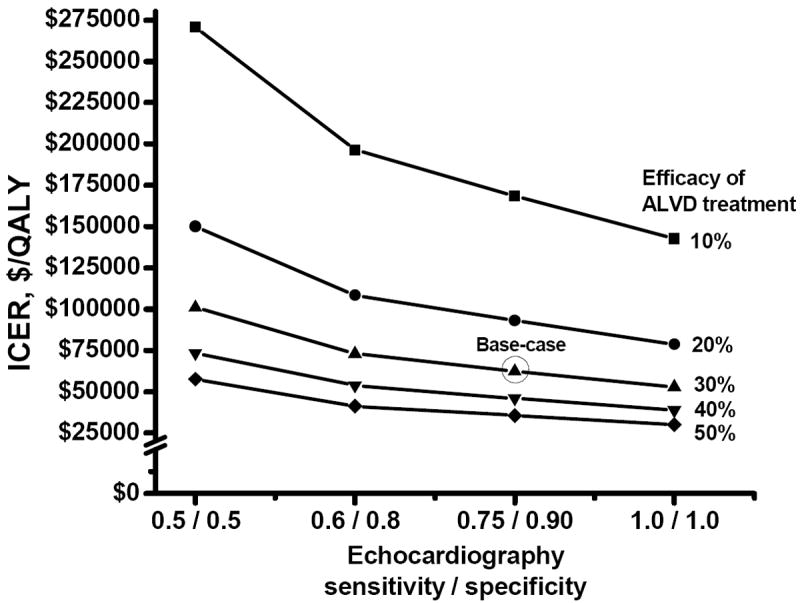
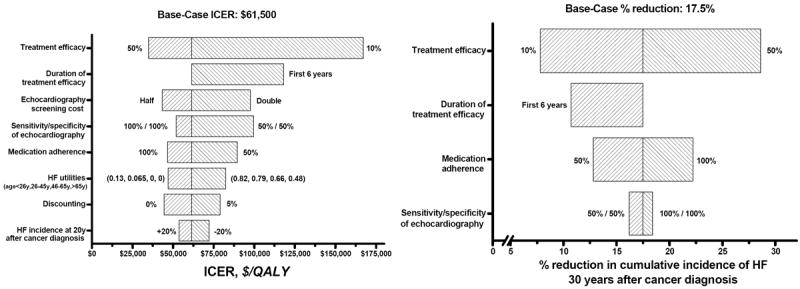
Results of base-case analysis: The COG guidelines versus no screening have an ICER of $61 500, extend life expectancy by 6 months and QALYs by 1.6 months, and reduce the cumulative incidence of heart failure by 18% at 30 years after cancer diagnosis. However, less frequent screenings are more cost-effective than the guidelines and maintain 80% of the health benefits.
Results of sensitivity analysis: The ICER was most sensitive to the magnitude of ALVD treatment efficacy; higher treatment efficacy resulted in lower ICER.
Limitation: Lifetime non-heart failure mortality and the cumulative incidence of heart failure more than 20 years after diagnosis were extrapolated; the efficacy of ACE inhibitor and β-blocker therapy in childhood cancer survivors with ALVD is undetermined (or unknown).
Conclusion: The COG guidelines could reduce the risk for heart failure in survivors at less than $100 000/QALY. Less frequent screening achieves most of the benefits and would be more cost-effective than the COG guidelines.
Conflict of interest statement
We declare that we have no conflict of interest.
Figures


Comment in
-
Cost-effectiveness of screening for asymptomatic left ventricular dysfunction in childhood cancer survivors.Ann Intern Med. 2014 May 20;160(10):731-2. doi: 10.7326/M14-0823. Ann Intern Med. 2014. PMID: 24842420 No abstract available.
References
-
- Lipshultz SE, Alvarez JA, Scully RE. Anthracycline associated cardiotoxicity in survivors of childhood cancer. Heart. 2008;94(4):525–33. - PubMed
-
- Lipshultz SE, Adams MJ, Colan SD, Constine LS, Herman EH, Hsu DT, et al. Long-term Cardiovascular Toxicity in Children, Adolescents, and Young Adults Who Receive Cancer Therapy: Pathophysiology, Course, Monitoring, Management, Prevention, and Research Directions: A Scientific Statement From the American Heart Association. Circulation. 2013 - PubMed
-
- Lipshultz SE, Colan SD, Gelber RD, Perez-Atayde AR, Sallan SE, Sanders SP. Late cardiac effects of doxorubicin therapy for acute lymphoblastic leukemia in childhood. N Engl J Med. 1991;324(12):808–15. - PubMed
-
- Lipshultz SE, Lipsitz SR, Sallan SE, Simbre VCn, Shaikh SL, Mone SM, et al. Long-term enalapril therapy for left ventricular dysfunction in doxorubicin-treated survivors of childhood cancer. J Clin Oncol. 2002;20(23):4517–22. - PubMed
-
- Lipshultz SE, Lipsitz SR, Sallan SE, Dalton VM, Mone SM, Gelber RD, et al. Chronic progressive cardiac dysfunction years after doxorubicin therapy for childhood acute lymphoblastic leukemia. J Clin Oncol. 2005;23(12):2629–36. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous