

The epidemiology and outcome of prehospital respiratory distress
- PMID: 24842506
- PMCID: PMC4247789
- DOI: 10.1111/acem.12380
The epidemiology and outcome of prehospital respiratory distress
Abstract
Objectives: Patients with respiratory distress often seek emergency medical care and are transported by emergency medical services (EMS). EMS encounters with patients in respiratory distress have not been well described. The study objective was to characterize the epidemiology of prehospital respiratory distress and subsequent patient outcomes.
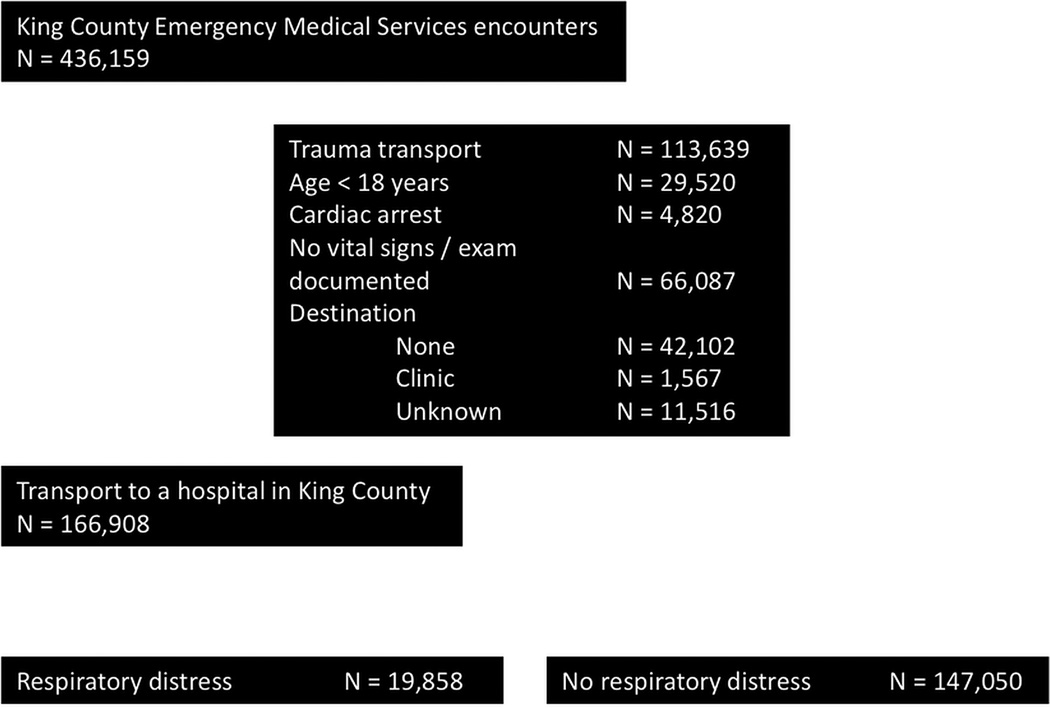
Methods: This was a population-based cohort study of noninjured adults transported by EMS to any of 16 hospitals between 2002 and 2006. EMS records were linked to hospital administrative data for encounters categorized by EMS personnel as primarily "respiratory distress" in nature. The authors described prehospital patient and encounter characteristics, interventions, hospital discharge diagnoses (using ICD-9-CM codes), and patient outcomes. The association between prehospital variables, defined a priori, and hospital admission were described using multivariable logistic regression.
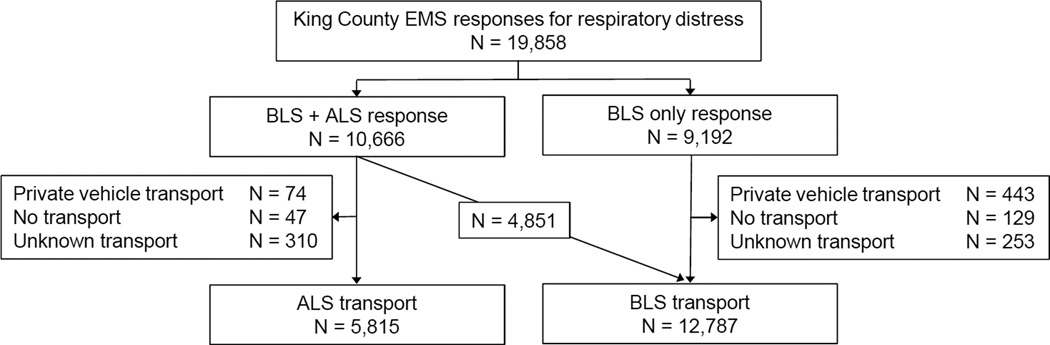
Results: There were 166,908 EMS encounters, of which 19,858 were for respiratory distress (11.9%, 95% confidence interval [CI] = 11.7% to 12.1%). Half of the patients were admitted to the hospital (n = 9,964), one-third of those required intensive care (n = 3,094), and 10% of hospitalized patients died prior to discharge (n = 948). Fifteen percent of hospitalized patients received invasive mechanical ventilation (n = 1,501), over half of whom were intubated during prehospital care (n = 896). The most common primary discharge diagnoses among prehospital respiratory distress patients admitted to the hospital were congestive heart failure (CHF; 16%), pneumonia (15%), chronic obstructive pulmonary disease (COPD; 13%), and acute respiratory failure (13%). Few EMS patients with respiratory distress were coded with a primary diagnosis of acute myocardial infarction (3.5%, n = 350) or underwent percutaneous coronary intervention (0.7%, n = 71). In a multivariable regression model, prehospital factors that were independently associated with hospital admission included initial respiratory rate (odds ratio [OR] = 1.29 for an increase in respiratory rate of five breaths/min, 95% CI = 1.24 to 1.35) and an encounter that originated at a nursing home (OR = 2.80, 95% CI = 2.28 to 3.43).
Conclusions: In a population-based cohort, EMS personnel commonly encounter prehospital respiratory distress among medical patients, many of whom require hospital admission to the intensive care unit. These data may help to inform targeted therapy or more efficient triage and transport decisions.
© 2014 by the Society for Academic Emergency Medicine.
Conflict of interest statement
The authors have no conflicts of interest to report.
Figures

References
-
- Centers for Disease Control and Prevention. [Accessed Jan 25, 2014];National Hospital Ambulatory Medical Care Survey (NHAMCS) - 2009 emergency department summary tables. Available at: http://www.cdc.gov/nchs/data/ahcd/nhamcs_emergency/2009_ed_web_tables.pdf.
-
- Braithwaite S, Perina D. Chapter 17. Dyspnea. In: JA Marx, RS Hockberger, RM Walls, et al., editors. Rosen's Emergency Medicine: Concepts and Clinical Practice. 7th. Philadelphia, PA: Elsevier; 1983. pp. 124–131.
-
- Hall MJ, Levant S, DeFrances CJ. Trends in inpatient hospital deaths: National Hospital Discharge Survey, 2000–2010. NCHS Data Brief. 2013;118:1–8. - PubMed
-
- Stiell IG, Spaite DW, Field B, et al. Advanced life support for out-of-hospital respiratory distress. N Engl J Med. 2007;356(21):2156–2164. - PubMed
-
- Pozner CN, Levine M, Shapiro N, Hanrahan JP. Concordance of field and emergency department assessment in the prehospital management of patients with dyspnea. Prehosp Emerg Care. 2003;7(4):440–444. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
