

Blood pressure control and cardiovascular outcomes in normal-weight, overweight, and obese hypertensive patients treated with three different antihypertensives in ALLHAT
- PMID: 24842697
- PMCID: PMC5592841
- DOI: 10.1097/HJH.0000000000000204
Blood pressure control and cardiovascular outcomes in normal-weight, overweight, and obese hypertensive patients treated with three different antihypertensives in ALLHAT
Abstract
Objective: Epidemiologically, there is a strong relationship between BMI and blood pressure (BP) levels. We prospectively examined randomization to first-step chlorthalidone, a thiazide-type diuretic; amlodipine, a calcium-channel blocker; and lisinopril, an angiotensin-converting enzyme inhibitor, on BP control and cardiovascular outcomes in a hypertensive cohort stratified by baseline BMI [kg/m(2); normal weight (BMI <25), overweight (BMI = 25-29.9), and obese (BMI >30)].
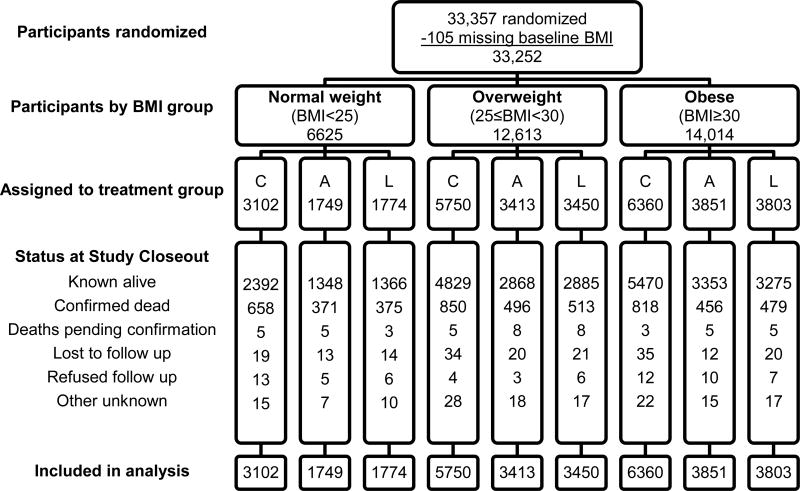
Methods: In a randomized, double-blind, practice-based Antihypertensive and Lipid-Lowering Treatment to Prevent Heart Attack Trial, 33,357 hypertensive participants, aged at least 55 years, were followed for an average of 4.9 years, for a primary outcome of fatal coronary heart disease or nonfatal myocardial infarction, and secondary outcomes of stroke, heart failure, combined cardiovascular disease, mortality, and renal failure.
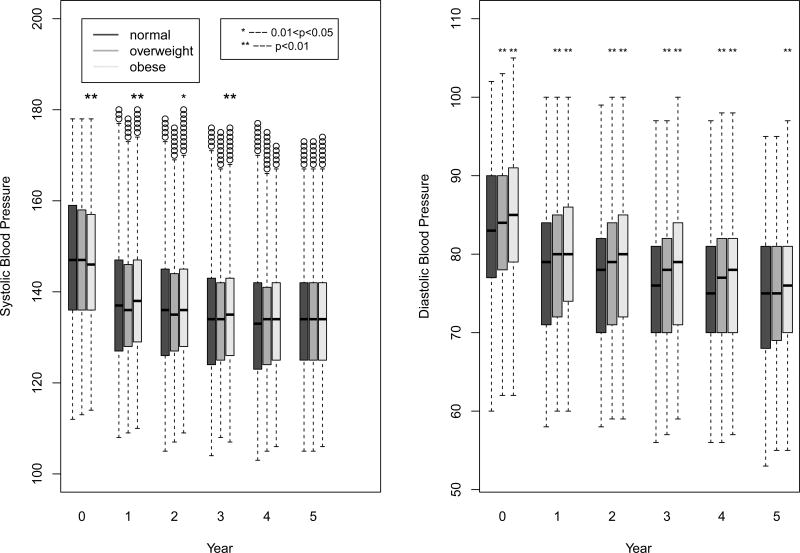
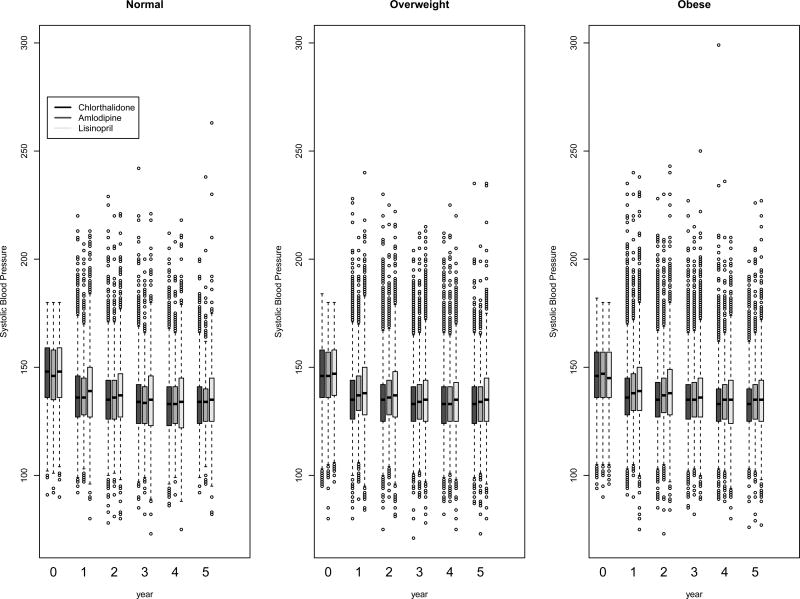
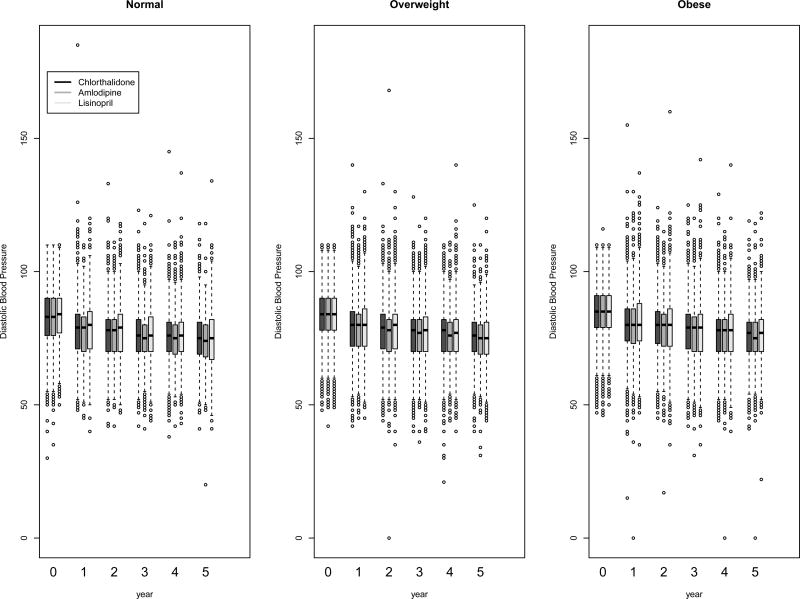
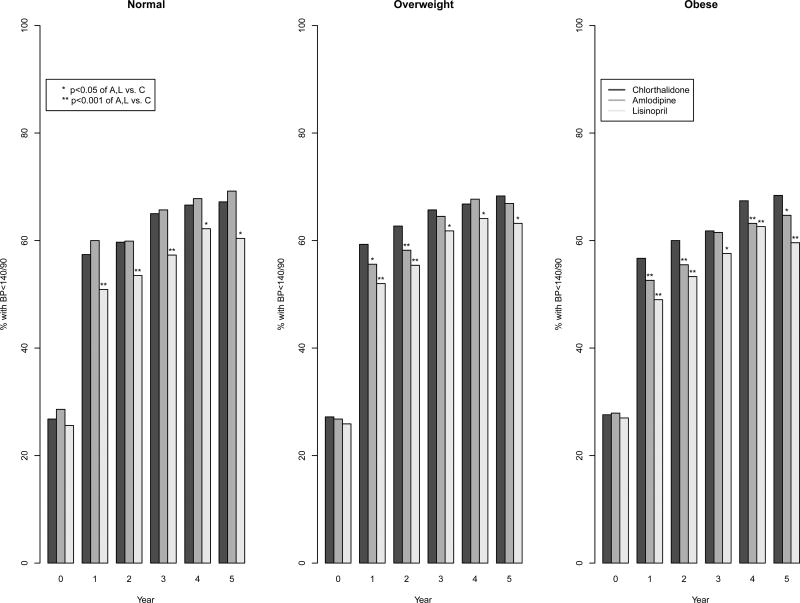
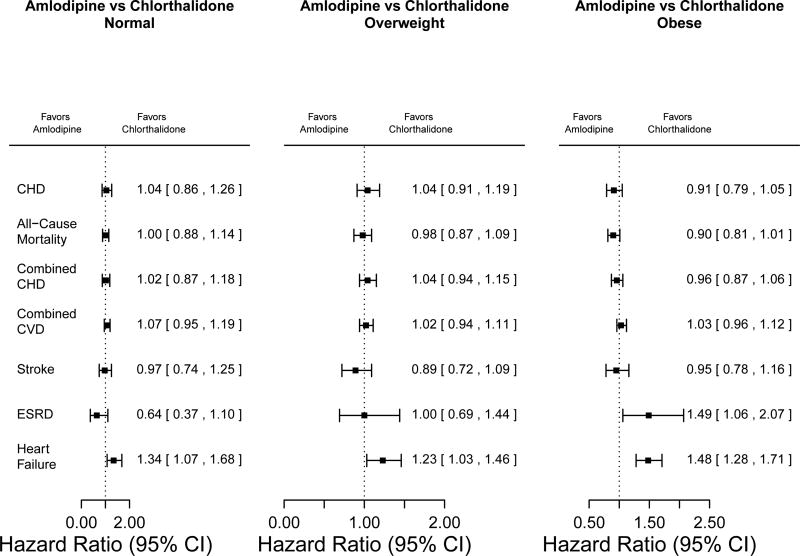
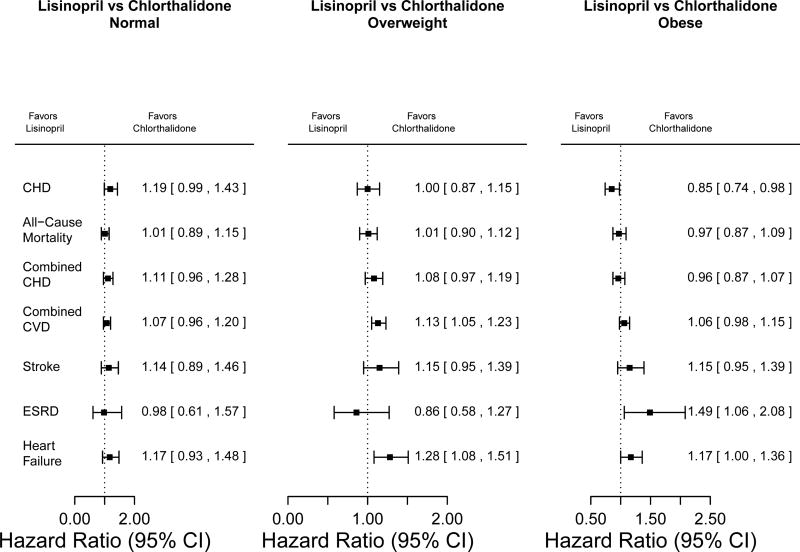
Results: Of participants, 37.9% were overweight and 42.1% were obese at randomization. For each medication, BP control (<140/90 mmHg) was equivalent in each BMI stratum. At the fifth year, 66.1, 66.5, and 65.1% of normal-weight, overweight, and obese participants, respectively, were controlled. Those randomized to chlorthalidone had highest BP control (67.2, 68.3, and 68.4%, respectively) and to lisinopril the lowest (60.4, 63.2, and 59.6%, respectively) in each BMI stratum. A significant interaction (P = 0.004) suggests a lower coronary heart disease risk in the obese for lisinopril versus chlorthalidone (hazard ratio 0.85, 95% confidence interval 0.74-0.98) and a significant interaction (P = 0.011) suggests a higher risk of end-stage renal disease for amlodipine versus chlorthalidone in obese participants (hazard ratio 1.49, 95% confidence interval 1.06-2.08). However, these results were not consistent among other outcomes.
Conclusion: BMI status does not modify the effects of antihypertensive medications on BP control or cardiovascular disease outcomes.
Trial registration: ClinicalTrials.gov NCT00000542.
Conflict of interest statement
Drs. Reisin, Graves, Yamal, Barzilay, Einhorn, Dart, Retta, and Saklayen, and Ms. Pressel have no conflicts to report. Dr. Davis has received honoraria from Takeda and Amgen.
Figures
Comment in
-
Antihypertensive treatments in obese patients: the Antihypertensive and Lipid Lowering Treatment to Prevent Heart Attack Trial experience.J Hypertens. 2014 Jul;32(7):1402-4. doi: 10.1097/HJH.0000000000000245. J Hypertens. 2014. PMID: 24984176 No abstract available.
References
-
- Brown CD, Higgins M, Donato KA, Rohde FC, Garrison R, Obarzanek E, et al. Body mass index and the prevalence of hypertension and dyslipidemia. Obes Res. 2000;8:605–619. - PubMed
-
- Stamler R, Stamler J, Riedlinger WF, Algera G, Roberts RH. Weight and blood pressure. Findings in hypertension screening of 1 million Americans. JAMA. 1978;240:1607–1610. - PubMed
-
- Pepine CJ, Handberg EM, Cooper-DeHoff RM, Marks RG, Kowey P, Messerli FH, et al. A calcium antagonist vs a non-calcium antagonist hypertension treatment strategy for patients with coronary artery disease. The International Verapamil-Trandolapril Study (INVEST): a randomized controlled trial. JAMA. 2003;290:2805–2816. - PubMed
-
- Dahlof B, Sever PS, Poulter NR, Wedel H, Beevers DG, Caulfield M, et al. Prevention of cardiovascular events with an antihypertensive regimen of amlodipine adding perindopril as required versus atenolol adding bendroflumethiazide as required, in the Anglo-Scandinavian Cardiac Outcomes Trial-Blood Pressure Lowering Arm (ASCOT-BPLA): a multicentre randomised controlled trial. Lancet. 2005;366:895–906. - PubMed
-
- Julius S, Nesbitt SD, Egan BM, Weber MA, Michelson EL, Kaciroti N, et al. Feasibility of treating prehypertension with an angiotensin-receptor blocker. N Engl J Med. 2006;354:1685–1697. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
