

The hepatitis C cascade of care: identifying priorities to improve clinical outcomes
- PMID: 24842841
- PMCID: PMC4026319
- DOI: 10.1371/journal.pone.0097317
The hepatitis C cascade of care: identifying priorities to improve clinical outcomes
Abstract
Background: As highly effective hepatitis C virus (HCV) therapies emerge, data are needed to inform the development of interventions to improve HCV treatment rates. We used simulation modeling to estimate the impact of loss to follow-up on HCV treatment outcomes and to identify intervention strategies likely to provide good value for the resources invested in them.
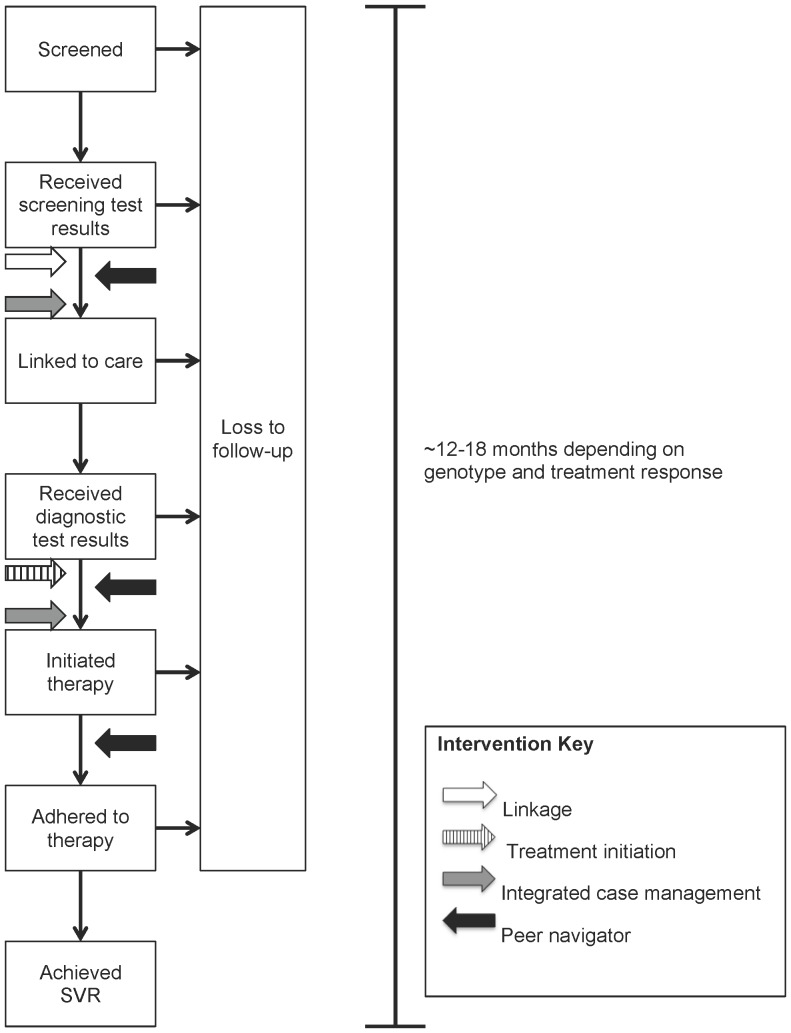
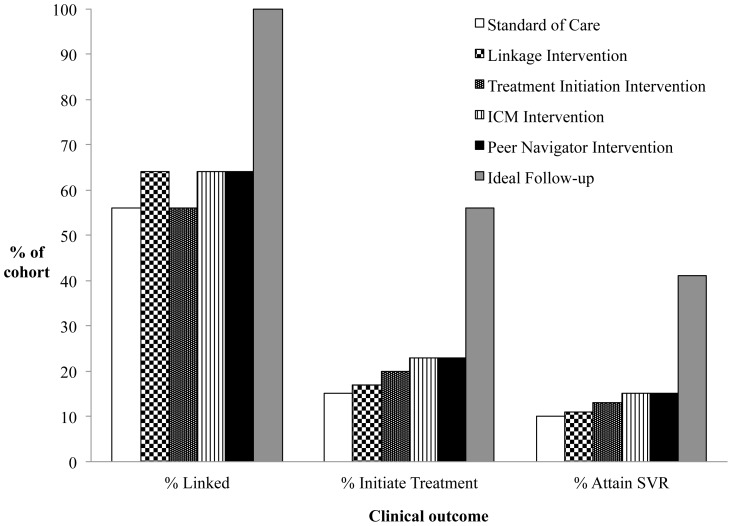
Methods: We used a Monte Carlo state-transition model to simulate a hypothetical cohort of chronically HCV-infected individuals recently screened positive for serum HCV antibody. We simulated four hypothetical intervention strategies (linkage to care; treatment initiation; integrated case management; peer navigator) to improve HCV treatment rates, varying efficacies and costs, and identified strategies that would most likely result in the best value for the resources required for implementation.
Main measures: Sustained virologic responses (SVRs), life expectancy, quality-adjusted life expectancy (QALE), costs from health system and program implementation perspectives, and incremental cost-effectiveness ratios (ICERs).
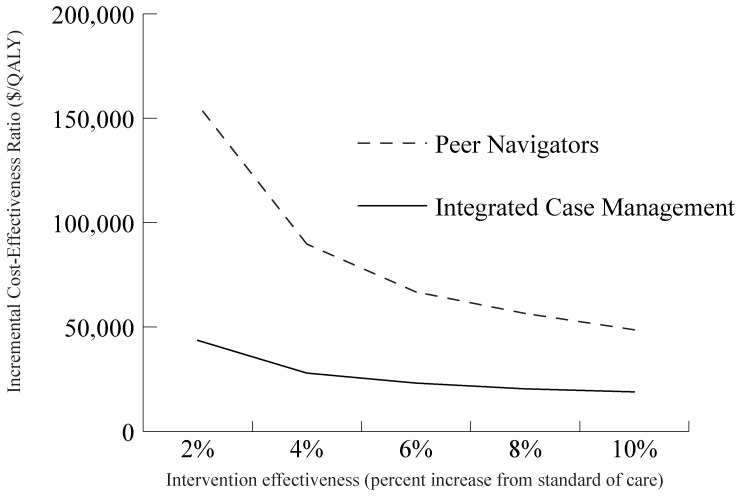
Results: We estimate that imperfect follow-up reduces the real-world effectiveness of HCV therapies by approximately 75%. In the base case, a modestly effective hypothetical peer navigator program maximized the number of SVRs and QALE, with an ICER compared to the next best intervention of $48,700/quality-adjusted life year. Hypothetical interventions that simultaneously addressed multiple points along the cascade provided better outcomes and more value for money than less costly interventions targeting single steps. The 5-year program cost of the hypothetical peer navigator intervention was $14.5 million per 10,000 newly diagnosed individuals.
Conclusions: We estimate that imperfect follow-up during the HCV cascade of care greatly reduces the real-world effectiveness of HCV therapy. Our mathematical model shows that modestly effective interventions to improve follow-up would likely be cost-effective. Priority should be given to developing and evaluating interventions addressing multiple points along the cascade rather than options focusing solely on single points.
Conflict of interest statement
Figures
References
-
- Smith BD, Morgan RL, Beckett GA, Falck-Ytter Y, Holtzman D, et al. (2012) Recommendations for the identification of chronic hepatitis C virus infection among persons born during 1945–1965. MMWR 61: 1–32. - PubMed
-
- Pearlman BL, Traub N (2011) Sustained virologic response to antiviral therapy for chronic hepatitis C virus infection: a cure and so much more. Clin Infect Dis 52: 889–900. - PubMed
-
- Swain MG, Lai MY, Shiffman ML, Cooksley WG, Zeuzem S, et al. (2010) A sustained virologic response is durable in patients with chronic hepatitis C treated with peginterferon alfa-2a and ribavirin. Gastroenterology 139: 1593–1601. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
