

Antiretroviral therapy and efficacy after virologic failure on first-line boosted protease inhibitor regimens
- PMID: 24842909
- PMCID: PMC4155445
- DOI: 10.1093/cid/ciu367
Antiretroviral therapy and efficacy after virologic failure on first-line boosted protease inhibitor regimens
Abstract
Background: Virologic failure (VF) on a first-line ritonavir-boosted protease inhibitor (PI/r) regimen is associated with low rates of resistance, but optimal management after failure is unknown.
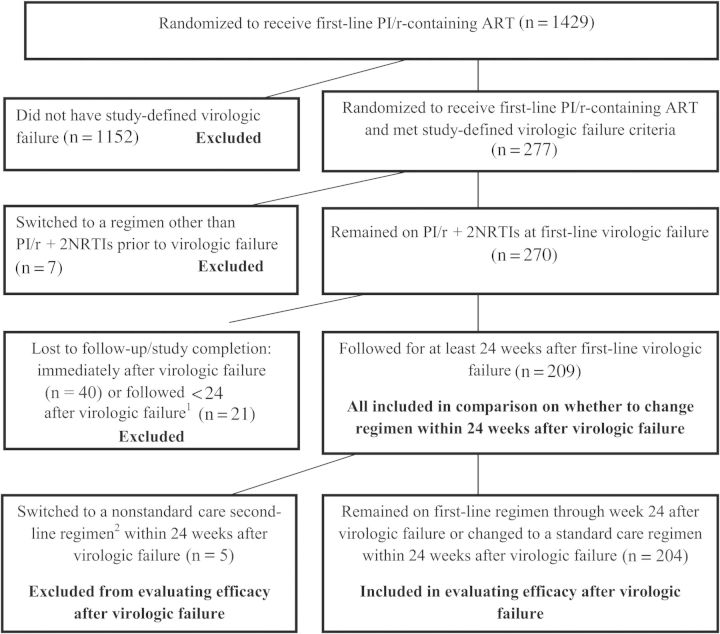
Methods: The analysis included participants in randomized trials who experienced VF on a first-line regimen of PI/r plus 2 nucleoside reverse transcriptase inhibitors (NRTIs) and had at least 24 weeks of follow-up after VF. Antiretroviral management and virologic suppression (human immunodeficiency virus type 1 [HIV-1] RNA <400 copies/mL) after VF were assessed.
Results: Of 209 participants, only 1 participant had major PI-associated treatment-emergent mutations at first-line VF. The most common treatment approach after VF (66%) was to continue the same regimen. The virologic suppression rate 24 weeks after VF was 64% for these participants, compared with 72% for those who changed regimens (P = .19). Participants remaining on the same regimen had lower NRTI resistance rates (11% vs 30%; P = .003) and higher CD4(+) cell counts (median, 275 vs 213 cells/µL; P = .005) at VF than those who changed. Among participants remaining on their first-line regimen, factors at or before VF significantly associated with subsequent virologic suppression were achieving HIV-1 RNA <400 copies/mL before VF (odds ratio [OR], 3.39 [95% confidence interval {CI}, 1.32-8.73]) and lower HIV-1 RNA at VF (OR for <10 000 vs ≥10 000 copies/mL, 3.35 [95% CI, 1.40-8.01]). Better adherence after VF was also associated with subsequent suppression (OR for <100% vs 100%, 0.38 [95% CI, .15-.97]). For participants who changed regimens, achieving HIV-1 RNA <400 copies/mL before VF also predicted subsequent suppression.
Conclusions: For participants failing first-line PI/r with no or limited drug resistance, remaining on the same regimen is a reasonable approach. Improving adherence is important to subsequent treatment success.
Keywords: antiretroviral therapy; first-line; protease inhibitor; virologic failure.
© The Author 2014. Published by Oxford University Press on behalf of the Infectious Diseases Society of America. All rights reserved. For Permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Panel on Antiretroviral Guidelines for Adults and Adolescents. Department of Health and Human Services; 2013. Guidelines for the use of antiretroviral agents in HIV-1 infected adults and adolescents. Available at: http://aidsinfo.nih.gov/contentfiles/lvguidelines/adultandadolescentgl.pdf . Accessed 28 January 2014.
-
- Thompson MA, Aberg JA, Hoy JF, et al. Antiretroviral treatment of adult HIV infection: 2012 recommendations of the International Antiviral Society-USA panel. JAMA. 2012;308:387–402. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
- UM1 AI069494/AI/NIAID NIH HHS/United States
- UM1 AI069472/AI/NIAID NIH HHS/United States
- UM1 AI069424/AI/NIAID NIH HHS/United States
- UM1 AI069456/AI/NIAID NIH HHS/United States
- UM1 AI069432/AI/NIAID NIH HHS/United States
- AI36214/AI/NIAID NIH HHS/United States
- UL1RR024996/RR/NCRR NIH HHS/United States
- UL1 TR000124/TR/NCATS NIH HHS/United States
- UM1AI069419/AI/NIAID NIH HHS/United States
- 1 UM1 AI068634/AI/NIAID NIH HHS/United States
- U01 AI069432/AI/NIAID NIH HHS/United States
- 1 UM1 AI068636/AI/NIAID NIH HHS/United States
- A1069424/PHS HHS/United States
- UM1AI069412/AI/NIAID NIH HHS/United States
- UM1 AI068636/AI/NIAID NIH HHS/United States
- UL1 RR024996/RR/NCRR NIH HHS/United States
- K24 AI064086/AI/NIAID NIH HHS/United States
- UM1 AI069412/AI/NIAID NIH HHS/United States
- UM1 AI068634/AI/NIAID NIH HHS/United States
- AI064086/AI/NIAID NIH HHS/United States
- P30 AI036214/AI/NIAID NIH HHS/United States
- UM1 AI069419/AI/NIAID NIH HHS/United States
- AI069432/AI/NIAID NIH HHS/United States
- UM1AI069472/AI/NIAID NIH HHS/United States
- UL1 TR000457/TR/NCATS NIH HHS/United States
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
