

Review
doi: 10.1161/CIRCULATIONAHA.113.001805.
Effect of maternal cardiovascular conditions and risk factors on offspring cardiovascular disease
Affiliations
- PMID: 24842934
- PMCID: PMC4053195
- DOI: 10.1161/CIRCULATIONAHA.113.001805
Item in Clipboard
Review
Effect of maternal cardiovascular conditions and risk factors on offspring cardiovascular disease
Circulation.
.
No abstract available
Keywords: cardiovascular diseases; embryonic and fetal development; fetal development; immunity; pregnancy; risk factors.
Conflict of interest statement
Figures
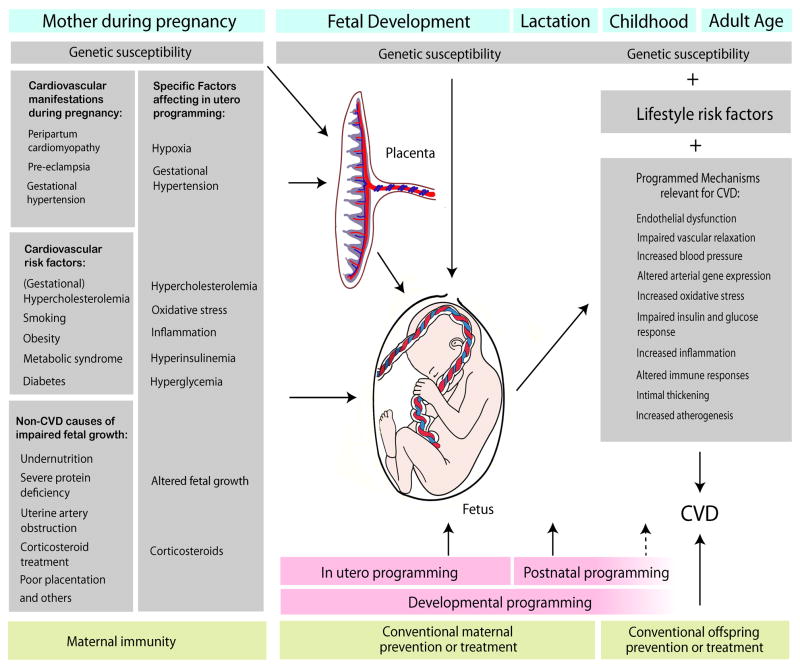
Current concept of developmental programming. Maternal causes of fetal programming include clinically relevant cardiovascular conditions during pregnancy, other CVD risk factors, such as chronic or gestational dysmetabolic conditions, and maternal factors unrelated to CVD that may influence offspring CVD by impairing fetal growth (left column). To date, only a limited number of specific factors have been proven to affect in utero programming (right column). Cardiovascular manifestations during pregnancy may program the fetus via hypoxia, hypertension, or altered fetal growth. Complex metabolic conditions in mothers may also influence programming via several specific factors. For example, the programming effects of maternal hypercholesterolemia may be due to hypercholesterolemia itself, increased oxidative stress, and inflammation. Similarly, obesity and metabolic syndrome may affect programming via hyperinsulinemia, hypercholesterolemia or dyslipidemia, increased oxidative stress, and increased inflammation. Maternal diabetes may act via hyperinsulinemia or hyperglycemia, as well as by altered fetal growth (macrosomia). Impaired fetal growth, or specific factors, such as corticosteroids, are thought to be responsible for programming by many non-CVD causes. Maternal genetic susceptibility may enhance the causes of fetal programming or affect placental function, whereas maternal adaptive immunity may result in protective immune programming, or protect against pathogenic programming by maternal factors, such as oxidative stress. Fetal programming may result from direct effects of maternal factors on the fetus, or be secondary to pathogenic effects on the placenta (see Figure 2 for details). Developmental programming is not limited to in utero programming, but continues after birth. In addition to maternal “environmental” factors, programming may be influenced by the genetic susceptibility of the fetus and by maternal treatment. In later childhood and adult age, the programmed mechanisms (gray box on the right) determine offspring CVD, together with the genetic susceptibility, lifestyle risk factors, and treatment. Note that the evidence for a protective effect of maternal immunity and treatments before or during pregnancy to date rests almost exclusively on experimental models.
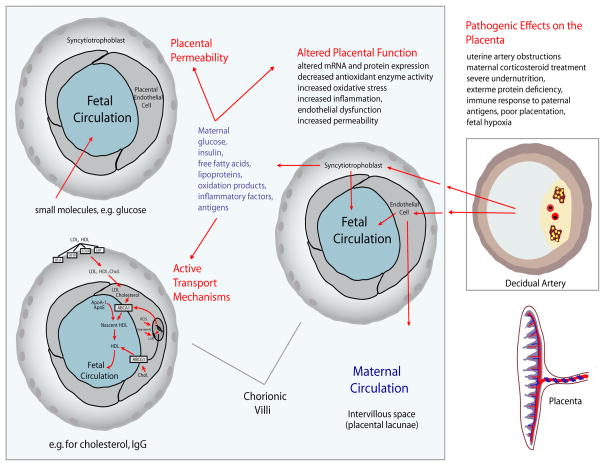
The role of the placenta in developmental programming. Chorionic villi are the site of maternal-fetal exchange. Maternal factors may program the fetus via placental permeability, by active transport across the placental barrier, or by influencing placental function. Placental permeability is regulated by fetal demand, increases during gestation, and is greatly increased by maternal pathogenic factors. Active transport mechanisms, e.g. for cholesterol, are also regulated and vary throughout gestation. Pathogenic effects on the placenta may result from non-CVD causes, e.g. uterine artery obstructions, poor placentation, immune rejection, or inflammation of decidual arteries. Maternal and placental factors may also affect the syncytiotrophoblast and endothelial cells, which in turn release pathogenic factors into the maternal or fetal circulation. (Cholesterol transport diagram modified from reference)
References
-
- Oyen N, Poulsen G, Boyd HA, Wohlfahrt J, Jensen PK, Melbye M. Recurrence of congenital heart defects in families. Circulation. 2009;120:295–301. - PubMed
-
- Ullmo S, Vial Y, Di BS, Roth-Kleiner M, Mivelaz Y, Sekarski N, Ruiz J, Meijboom EJ. Pathologic ventricular hypertrophy in the offspring of diabetic mothers: a retrospective study. Eur Heart J. 2007;28:1319–1325. - PubMed
-
- Cedergren MI, Kallen BA. Maternal obesity and infant heart defects. Obes Res. 2003;11:1065–1071. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
