

Tropospheric winds from northeastern China carry the etiologic agent of Kawasaki disease from its source to Japan
- PMID: 24843117
- PMCID: PMC4050536
- DOI: 10.1073/pnas.1400380111
Tropospheric winds from northeastern China carry the etiologic agent of Kawasaki disease from its source to Japan
Abstract
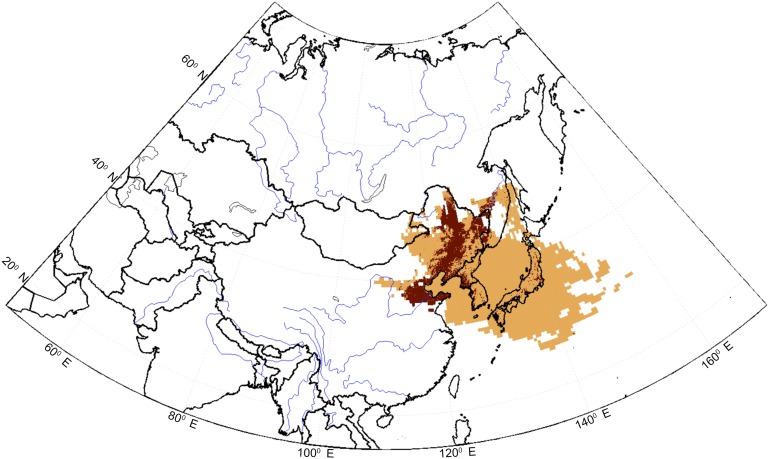
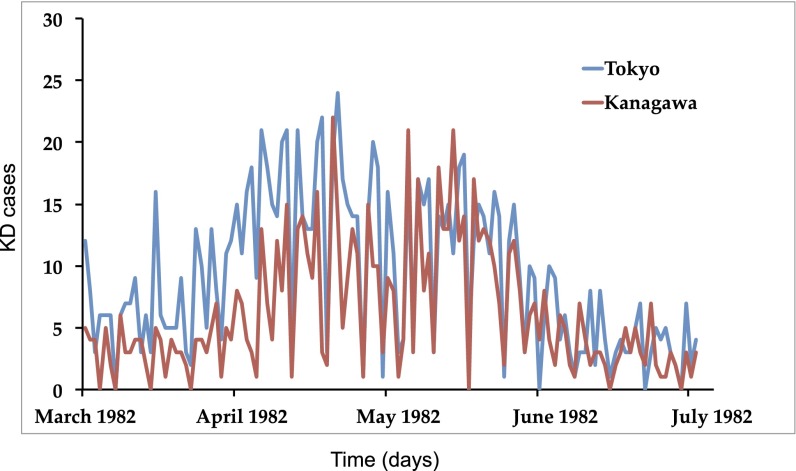
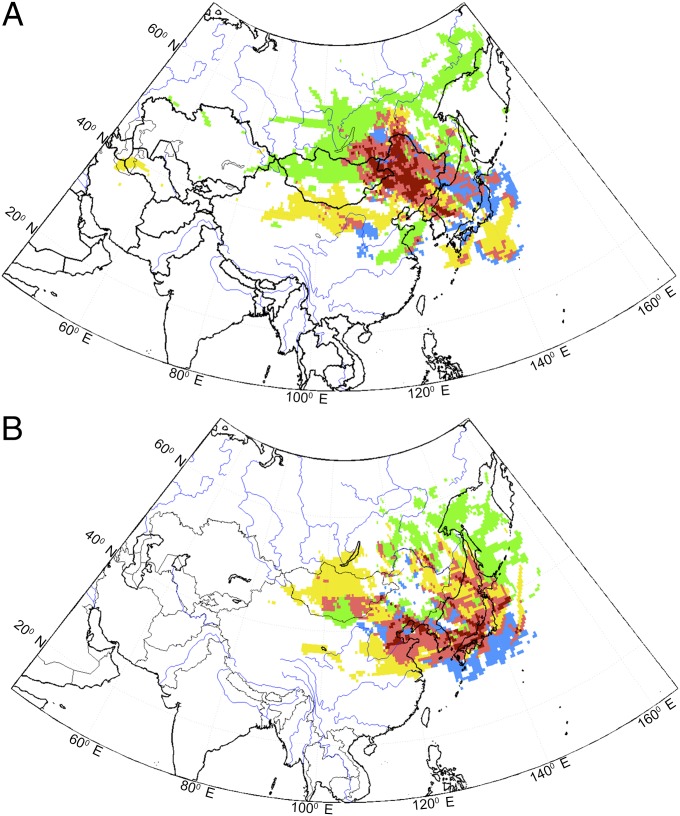
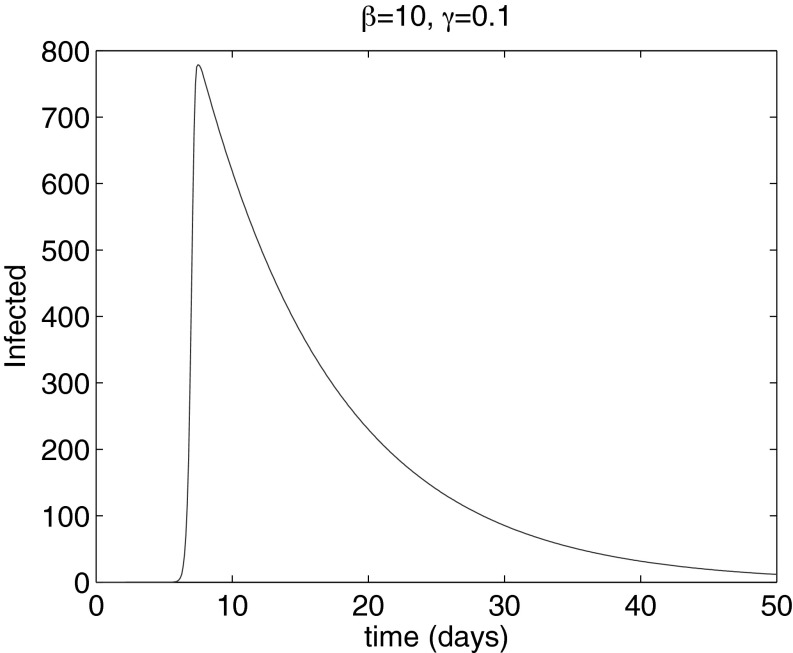
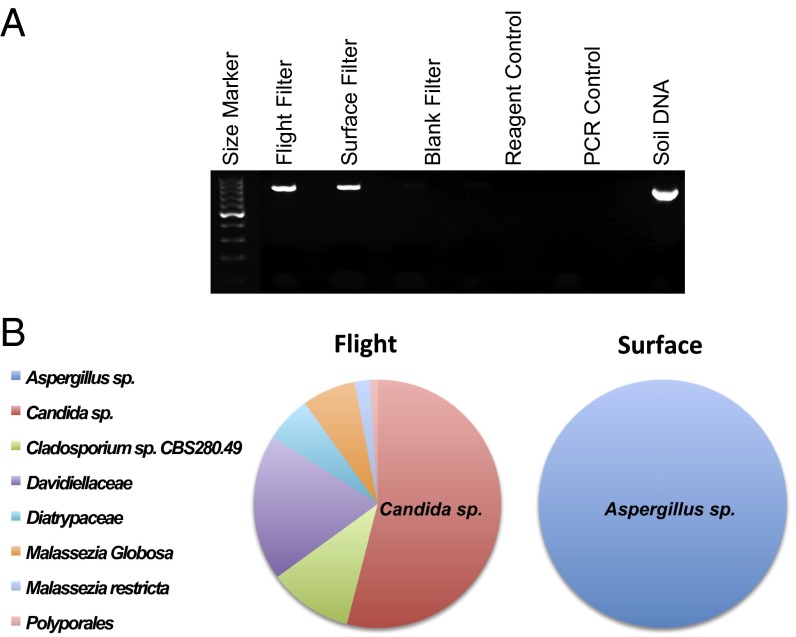
Evidence indicates that the densely cultivated region of northeastern China acts as a source for the wind-borne agent of Kawasaki disease (KD). KD is an acute, coronary artery vasculitis of young children, and still a medical mystery after more than 40 y. We used residence times from simulations with the flexible particle dispersion model to pinpoint the source region for KD. Simulations were generated from locations spanning Japan from days with either high or low KD incidence. The postepidemic interval (1987-2010) and the extreme epidemics (1979, 1982, and 1986) pointed to the same source region. Results suggest a very short incubation period (<24 h) from exposure, thus making an infectious agent unlikely. Sampling campaigns over Japan during the KD season detected major differences in the microbiota of the tropospheric aerosols compared with ground aerosols, with the unexpected finding of the Candida species as the dominant fungus from aloft samples (54% of all fungal strains). These results, consistent with the Candida animal model for KD, provide support for the concept and feasibility of a windborne pathogen. A fungal toxin could be pursued as a possible etiologic agent of KD, consistent with an agricultural source, a short incubation time and synchronized outbreaks. Our study suggests that the causative agent of KD is a preformed toxin or environmental agent rather than an organism requiring replication. We propose a new paradigm whereby an idiosyncratic immune response, influenced by host genetics triggered by an environmental exposure carried on winds, results in the clinical syndrome known as acute KD.
Keywords: FLEXPART; agriculture; cereal croplands; heart disease; northeastern China source.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Kawasaki T, Kosaki F, Okawa S, Shigematsu I, Yanagawa H. A new infantile acute febrile mucocutaneous lymph node syndrome (MLNS) prevailing in Japan. Pediatrics. 1974;54(3):271–276. - PubMed
-
- Cimaz R, Falcini F. An update on Kawasaki disease. Autoimmun Rev. 2003;2(5):258–263. - PubMed
-
- Rowley AH, et al. IgA plasma cell infiltration of proximal respiratory tract, pancreas, kidney, and coronary artery in acute Kawasaki disease. J Infect Dis. 2000;182(4):1183–1191. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
