

Primary squamous cell carcinoma of the external auditory canal: surgical treatment and long-term outcomes
- PMID: 24843224
- PMCID: PMC4025180
Primary squamous cell carcinoma of the external auditory canal: surgical treatment and long-term outcomes
Abstract
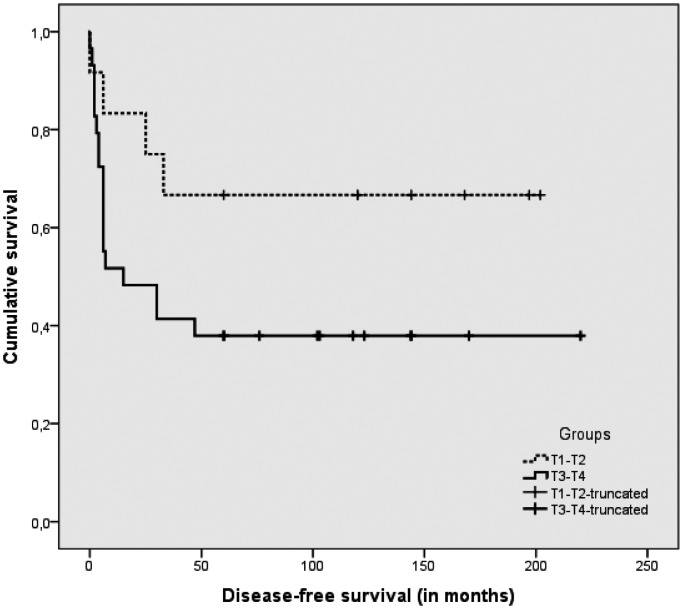
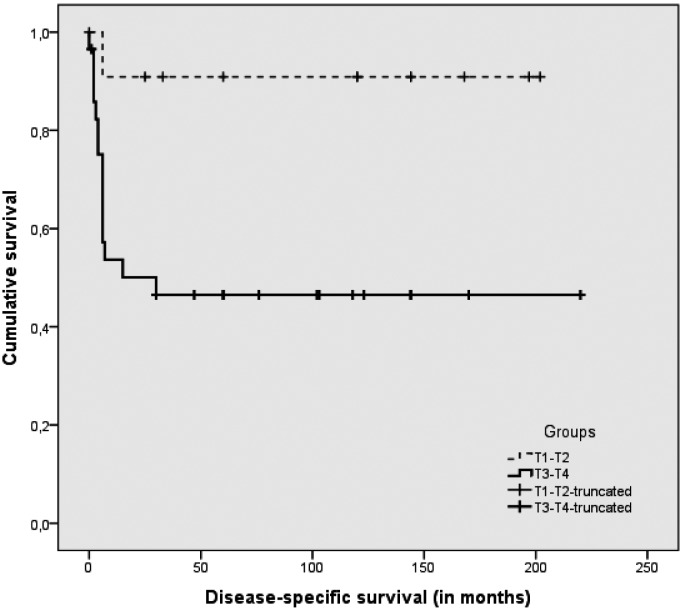
This study was conducted on patients with squamous cell carcinoma of the external auditory canal and temporal bone treated with surgery alone or surgery plus postoperative radiotherapy. It was designed as a retrospective investigation with complete long-term follow-up covering the years from 1983 to 2008. The setting was a tertiary referral centre. Forty-one consecutive cases underwent surgery involving en bloc lateral or subtotal temporal bone resection, parotidectomy and neck dissection plus radiotherapy in advanced cases. The Pittsburgh staging system was adopted. No cases were lost to follow-up, which ranged from 2 to 220 months, while for survivors ranged from 60 to 220 months and included clinical examinations and imaging. Outcome was expressed as NED (no evidence of disease), DOC (dead of other causes), DOD (dead of disease), AWD (alive with disease), disease-free survival (DFS) and disease-specific survival (DSS). Results were expressed with raw data and Kaplan Meyer curves. Patients with T1 and T2 disease had a DFS of 67% and a DSS of 92%. For T3 and T4 cases, the DFS was 41% and DSS was 48%. All treatment failures were due to local recurrences. The cases classified as T4 because the lesion extended from the cartilage canal to the periauricular soft tissues, or from the anterior wall to the parotid space, had a better outcome than the other T4 cases: this different prognosis suggests the need to stage tumours differently. Nodal disease coincided with a worse outcome due to local recurrence.
L'obiettivo di questo lavoro è valutare i risultati a lungo termine del trattamento chirurgico e chirurgico/radioterapico nel carcinoma spinocellulare primitivo del condotto uditivo esterno-osso temporale. Lo studio consiste in una analisi retrospettiva con follow-up a lungo termine. I casi chirurgici sono stati trattati tutti in un centro terziario di riferimento negli anni dal 1983 al 2008. Sono stati analizzati 41 casi di tumore spinocellulare primitivo del condotto uditivo esterno, trattati chirurgicamente con blocco resezione laterale o subtotale del temporale, parotidectomia, svuotamento laterocervicale elettivo o terapeutico. Abbiamo utilizzato la classificazione di Pittsburgh. Il follow-up si estende da 2 mesi a 220 mesi e, per quelli sopravvissuti, da un minimo di 60 mesi a 220 mesi. I risultati sono stati espressi come NED, DOD, DOC e AWD (non-evidenza di malattia, morto per malattia, morto per altre cause e vivo con malattia), con dati crudi e con curve di Kaplan Meyer. I T1-T2 hanno una sopravvivenza libera da malattia del 67%, ed una sopravvivenza specifica per malattia del 92%. I T3-T4 hanno una sopravvivenza libera da malattia del 41% e una sopravvivenza specifica del 48%. Tutti gli insuccessi sono avvenuti per recidiva locale. I casi stadiati come T4 per estensione da cartilagine ai tessuti molli o dalla parete anteriore alla parotide hanno avuto una miglior prognosi rispetto ai T4 con differente estensione mediale, inferiore o posteriore. Questa differenza di prognosi suggerisce la necessità di un cambio della stadiazione. Il coinvolgimento linfonodale implica una prognosi peggiore ma per recidiva locale e non regionale.
Keywords: Carcinoma of the ear; Lateral skull base surgery; Temporal bone resections; Temporal bone tumour.
Figures
References
-
- Pensak ML, Gleich LL, Gluckman JK, et al. Temporal bone carcinoma: contemporary perspectives in the skull base surgical era. Laryngoscope. 1996;106:1234–1237. - PubMed
-
- Arena S, Keen M. Carcinoma of the middle ear and temporal bone. Am J Otol. 1998;9:351–356. - PubMed
-
- Leonetti JP, Smith PG, Kletzker GR, et al. Invasion patterns of advanced temporal bone malignancies. Am J Otol. 2000;122:882–886. - PubMed
-
- Grandis JR, Hirsch B, Yu VL. Simultaneous presentation of malignant external otitis and temporal bone cancer. Arch Otolaryngol Head Neck Surg. 1993;119:687–689. - PubMed
-
- Al-Shihabi A. Carcinoma of temporal bone presenting as malignant otitis externa. J Laryngol Otol. 1992:908–910. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials