

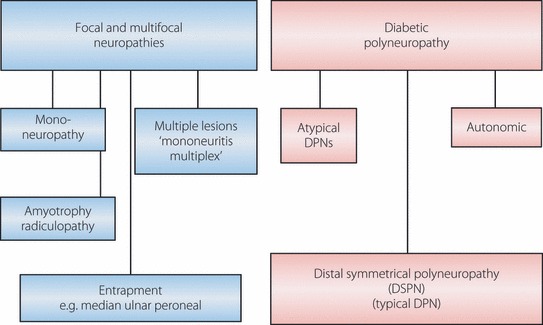
Recent advances in the management of diabetic distal symmetrical polyneuropathy
- PMID: 24843458
- PMCID: PMC4008012
- DOI: 10.1111/j.2040-1124.2010.00083.x
Recent advances in the management of diabetic distal symmetrical polyneuropathy
Abstract
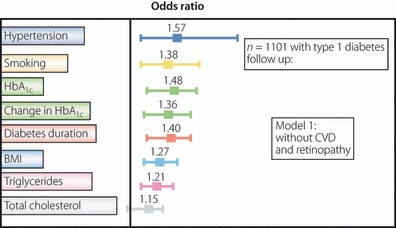
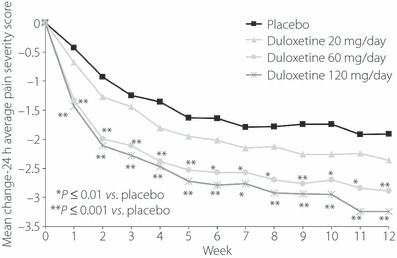
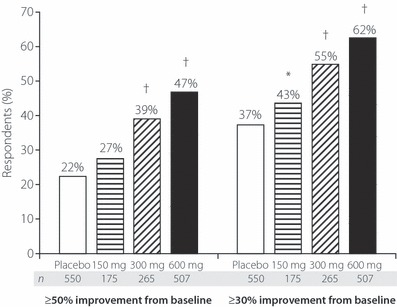
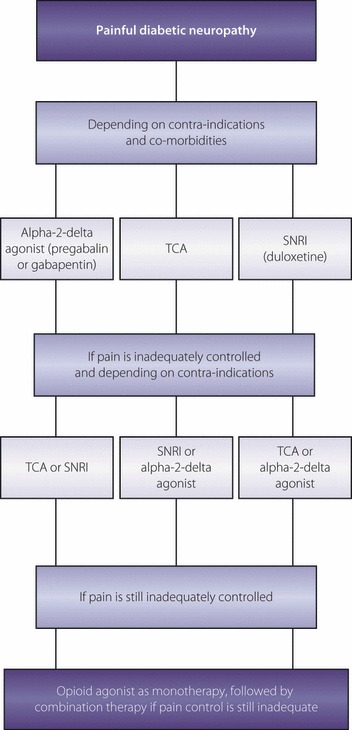
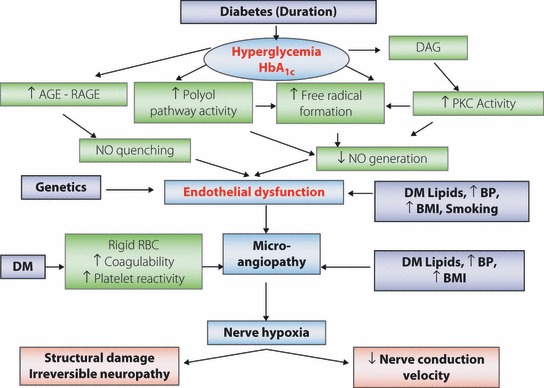
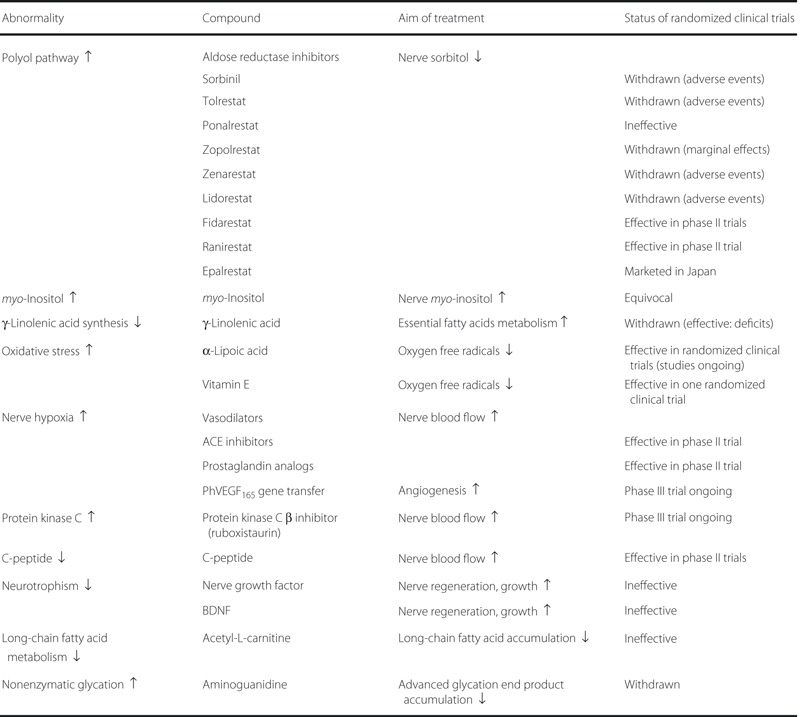
There is now little doubt that poor blood glucose control is an important risk factor for the development of diabetic peripheral neuropathy (DPN). Furthermore, traditional cardiovascular risk factors for macrovascular disease appear to be associated with an increased risk of DPN. The recently established International Expert Group on Diabetic Neuropathy has recommended new criteria for the diagnosis of DPN in the context of clinical and research settings. Studies in experimental diabetes examining the pathogenesis of DPN have identified a number of metabolic abnormalities including polyol pathway hyperactivity, increased advanced glycation end-point formation, alterations in the protein kinase C beta pathway through diacylglycerol and oxidative stress. There is now strong evidence implicating nerve ischemia as the cause of DPN. Studies in human and animal models have shown reduced nerve perfusion and endoneurial hypoxia. These endoneurial microvascular changes strongly correlate with clinical severity and the degree of nerve-fiber pathology. Unfortunately, many compounds that have been effective in animal models of neuropathy have not been successful in human diabetic neuropathy. The only compounds found to be efficacious in human diabetic neuropathy, and are in clinical use, are the anti-oxidant, α-lipoic acid and the aldose reductase inhibitor, epalrestat. Overall, the evidence emphasizes the importance of vascular dysfunction, driven by metabolic change, in the etiology of DPN, and highlights potential therapeutic approaches. Epidemiological data on diabetic painful neuropathic pain (DPNP) are limited. In one population-based study, the prevalence of DPNP, as assessed by a structured questionnaire and examination, was estimated at 16%. It was notable that, of these patients, 12.5% had never reported symptoms to their doctor and 39% had never received treatment for their pain. Thus, despite being common, DPNP continues to be underdiagnosed and undertreated. Pharmacological treatment of DPNP include tricyclic compounds, serotonin noradrenalin reuptake inhibitors, the anti-oxidant α-lipoic acid, anticonvulsants, opiates, membrane stabilizers, topical capsaicin and so on. Management of the patient with DPNP must be tailored to individual requirements and will depend on the presence of other comorbidities. (J Diabetes Invest, doi: 10.1111/j.2040-1124.2010.00083.x).
Keywords: Diabetic neuropathy; Diabetic peripheral neuropathy; Painful diabetic neuropathy.
Figures
Similar articles
-
Advances in the management of diabetic peripheral neuropathy.Curr Opin Support Palliat Care. 2009 Jun;3(2):136-43. doi: 10.1097/SPC.0b013e32832b7df5. Curr Opin Support Palliat Care. 2009. PMID: 19421063 Review.
-
Advances in the epidemiology, pathogenesis and management of diabetic peripheral neuropathy.Diabetes Metab Res Rev. 2012 Feb;28 Suppl 1:8-14. doi: 10.1002/dmrr.2239. Diabetes Metab Res Rev. 2012. PMID: 22271716 Review.
-
Painful diabetic peripheral neuropathy: consensus recommendations on diagnosis, assessment and management.Diabetes Metab Res Rev. 2011 Oct;27(7):629-38. doi: 10.1002/dmrr.1225. Diabetes Metab Res Rev. 2011. PMID: 21695762
-
Diabetic painful neuropathy: current and future treatment options.Drugs. 2007;67(4):569-85. doi: 10.2165/00003495-200767040-00006. Drugs. 2007. PMID: 17352515 Review.
-
Update on the management of diabetic polyneuropathies.Diabetes Metab Syndr Obes. 2011;4:289-305. doi: 10.2147/DMSO.S11324. Epub 2011 Jul 21. Diabetes Metab Syndr Obes. 2011. PMID: 21887102 Free PMC article.
Cited by
-
Prevalence and Determinants of Peripheral Neuropathy among Type 2 Adult Diabetes Patients Attending Jimma University Medical Center, Southwest Ethiopia, 2019, an Institutional-Based Cross-Sectional Study.J Diabetes Res. 2020 Jun 29;2020:9562920. doi: 10.1155/2020/9562920. eCollection 2020. J Diabetes Res. 2020. PMID: 32685561 Free PMC article.
-
Carvedilol Exerts Neuroprotective Effect on Rat Model of Diabetic Neuropathy.Front Pharmacol. 2021 Apr 13;12:613634. doi: 10.3389/fphar.2021.613634. eCollection 2021. Front Pharmacol. 2021. PMID: 33927613 Free PMC article.
-
Assessment of peripheral neuropathy in type 2 diabetes by diffusion tensor imaging.Quant Imaging Med Surg. 2022 Jan;12(1):395-405. doi: 10.21037/qims-21-126. Quant Imaging Med Surg. 2022. PMID: 34993088 Free PMC article.
-
Quantitative thermal testing as a screening and follow-up tool for diabetic sensorimotor polyneuropathy in patients with type 2 diabetes and prediabetes.Front Neurosci. 2023 Mar 27;17:1115242. doi: 10.3389/fnins.2023.1115242. eCollection 2023. Front Neurosci. 2023. PMID: 37051142 Free PMC article.
-
The Interaction of Diabetic Peripheral Neuropathy and Carpal Tunnel Syndrome.Hand (N Y). 2023 Jan;18(1_suppl):43S-47S. doi: 10.1177/15589447211014607. Epub 2021 May 25. Hand (N Y). 2023. PMID: 34032176 Free PMC article.
References
-
- Dyck PJ, Kratz KM, Karnes JL, et al. The prevalence by staged severity of various types of diabetic neuropathy, retinopathy, and nephropathy in a population‐based cohort: the Rochester Diabetic Neuropathy Study. Neurology 1993; 43: 817–824 - PubMed
-
- Forsblom CM, Sane T, Groop PH, et al. Risk factors for mortality in type II (non‐insulin‐dependent) diabetes: evidence of a role for neuropathy and a protective effect of HLA‐DR4. Diabetologia 1998; 4: 1253–1262 - PubMed
-
- Quattrini C, Tesfaye S. Understanding the impact of painful diabetic neuropathy. Diabetes Metab Res Rev 2003; 19: S2–S8 - PubMed
Publication types
LinkOut - more resources
Full Text Sources
