

Neuropsychological criteria for mild cognitive impairment improves diagnostic precision, biomarker associations, and progression rates
- PMID: 24844687
- PMCID: PMC4133291
- DOI: 10.3233/JAD-140276
Neuropsychological criteria for mild cognitive impairment improves diagnostic precision, biomarker associations, and progression rates
Abstract
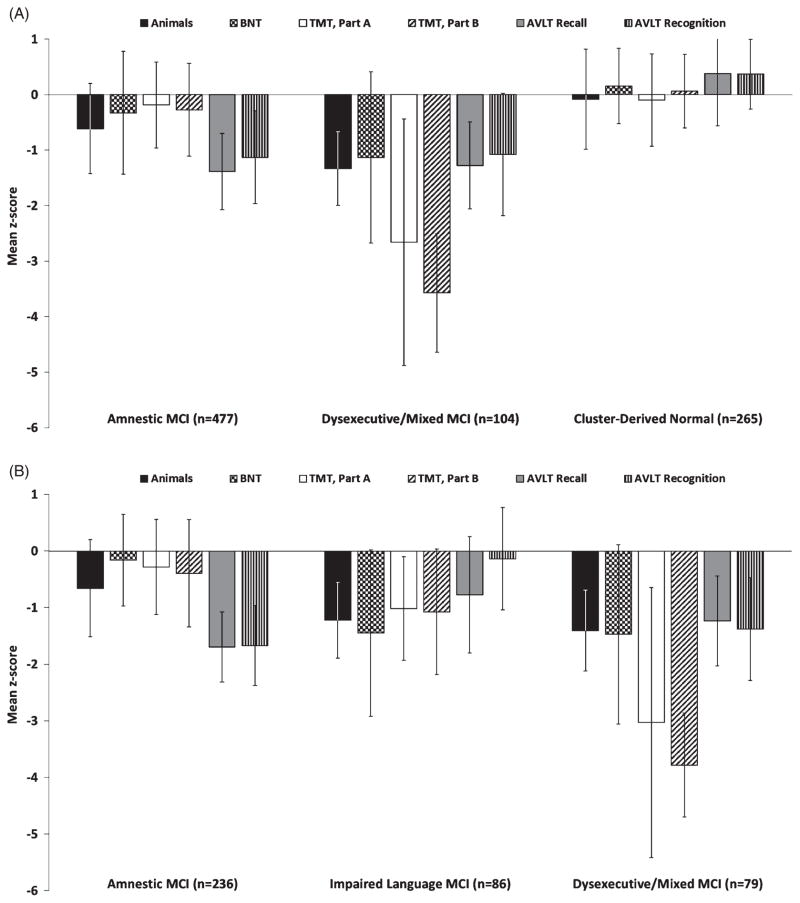
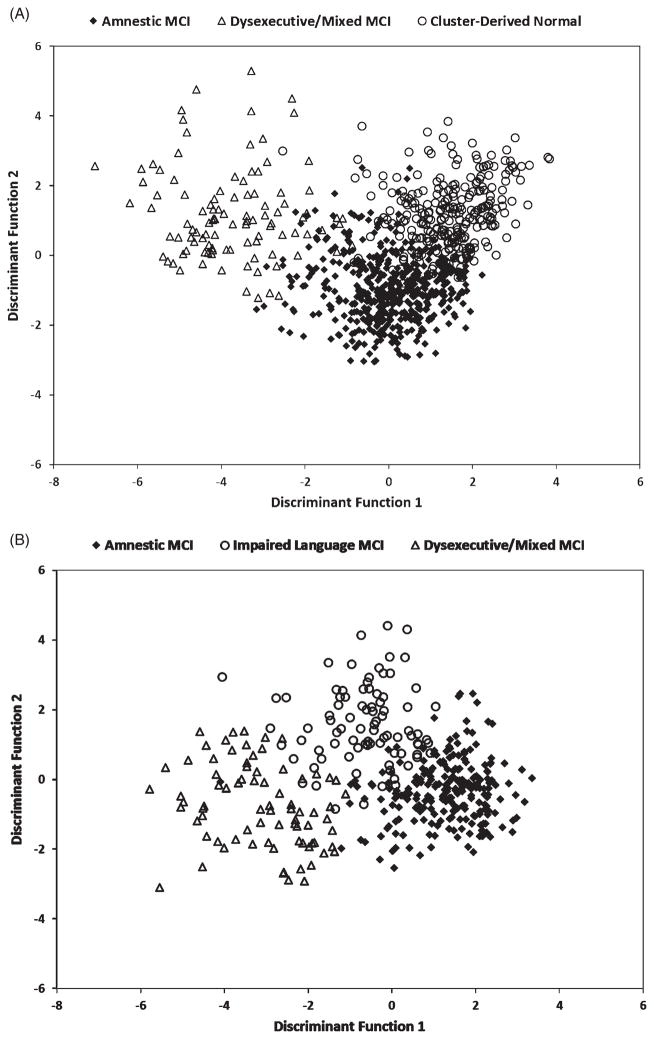
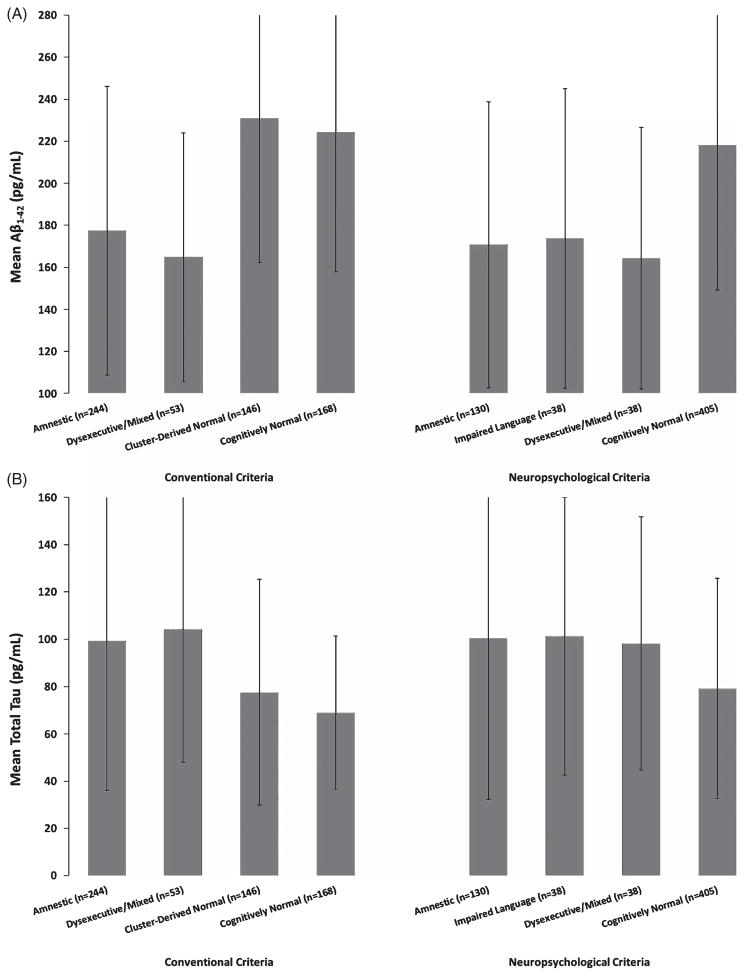
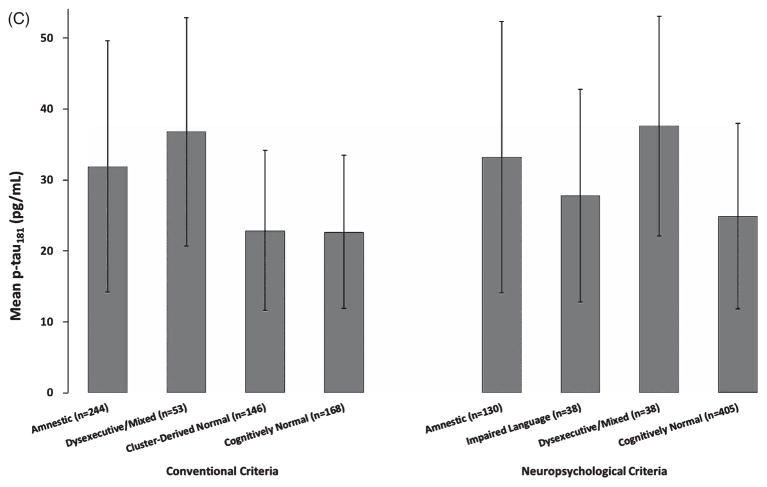
We compared two methods of diagnosing mild cognitive impairment (MCI): conventional Petersen/Winblad criteria as operationalized by the Alzheimer's Disease Neuroimaging Initiative (ADNI) and an actuarial neuropsychological method put forward by Jak and Bondi designed to balance sensitivity and reliability. 1,150 ADNI participants were diagnosed at baseline as cognitively normal (CN) or MCI via ADNI criteria (MCI: n = 846; CN: n = 304) or Jak/Bondi criteria (MCI: n = 401; CN: n = 749), and the two MCI samples were submitted to cluster and discriminant function analyses. Resulting cluster groups were then compared and further examined for APOE allelic frequencies, cerebrospinal fluid (CSF) Alzheimer's disease (AD) biomarker levels, and clinical outcomes. Results revealed that both criteria produced a mildly impaired Amnestic subtype and a more severely impaired Dysexecutive/Mixed subtype. The neuropsychological Jak/Bondi criteria uniquely yielded a third Impaired Language subtype, whereas conventional Petersen/Winblad ADNI criteria produced a third subtype comprising nearly one-third of the sample that performed within normal limits across the cognitive measures, suggesting this method's susceptibility to false positive diagnoses. MCI participants diagnosed via neuropsychological criteria yielded dissociable cognitive phenotypes, significant CSF AD biomarker associations, more stable diagnoses, and identified greater percentages of participants who progressed to dementia than conventional MCI diagnostic criteria. Importantly, the actuarial neuropsychological method did not produce a subtype that performed within normal limits on the cognitive testing, unlike the conventional diagnostic method. Findings support the need for refinement of MCI diagnoses to incorporate more comprehensive neuropsychological methods, with resulting gains in empirical characterization of specific cognitive phenotypes, biomarker associations, stability of diagnoses, and prediction of progression. Refinement of MCI diagnostic methods may also yield gains in biomarker and clinical trial study findings because of improvements in sample compositions of 'true positive' cases and removal of 'false positive' cases.
Keywords: Alzheimer's Disease Neuroimaging Initiative; Alzheimer's disease; biomarker; cluster analysis; dementia; mild cognitive impairment; neuropsychology; progression.
Figures
References
-
- McKhann G, Drachman D, Folstein M, Katzman R, Price D, Stadlan EM. Clinical diagnosis of Alzheimer’s disease: Report of the NINCDS-ADRDA Work Group under the auspices of Department of Health and Human Services Task Force on Alzheimer’s Disease. Neurology. 1984;34:939–944. - PubMed
-
- Flicker C, Ferris SH, Reisberg B. Mild cognitive impairment in the elderly: Predictors of dementia. Neurology. 1991;41:1006–1009. - PubMed
-
- Petersen RC, Smith GE, Waring SC, Ivnik RJ, Tangalos EG, Kokmen E. Mild cognitive impairment: Clinical characterization and outcome. Arch Neurol. 1999;56:303–308. - PubMed
-
- Petersen RC, Morris JC. Mild cognitive impairment as a clinical entity and treatment target. Arch Neurol. 2005;62:1160–1163. - PubMed
-
- Winblad B, Palmer K, Kivipelto M, Jelic V, Fratiglioni L, Wahlund LO, Nordberg A, Bäckman L, Albert M, Almkvist O, Arai H, Basun H, Blennow K, de Leon M, DeCarli C, Erkinjuntti T, Giacobini E, Graff C, Hardy J, Jack C, Jorm A, Ritchie K, van Duijn C, Visser P, Petersen RC. Mild cognitive impairment beyond controversies, towards a consensus: Report of the International Working Group on Mild Cognitive Impairment. J Intern Med. 2004;256:240–246. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
