

Fracture reduction and primary ankle arthrodesis: a reliable approach for severely comminuted tibial pilon fracture
- PMID: 24844887
- PMCID: PMC4397758
- DOI: 10.1007/s11999-014-3683-x
Fracture reduction and primary ankle arthrodesis: a reliable approach for severely comminuted tibial pilon fracture
Abstract
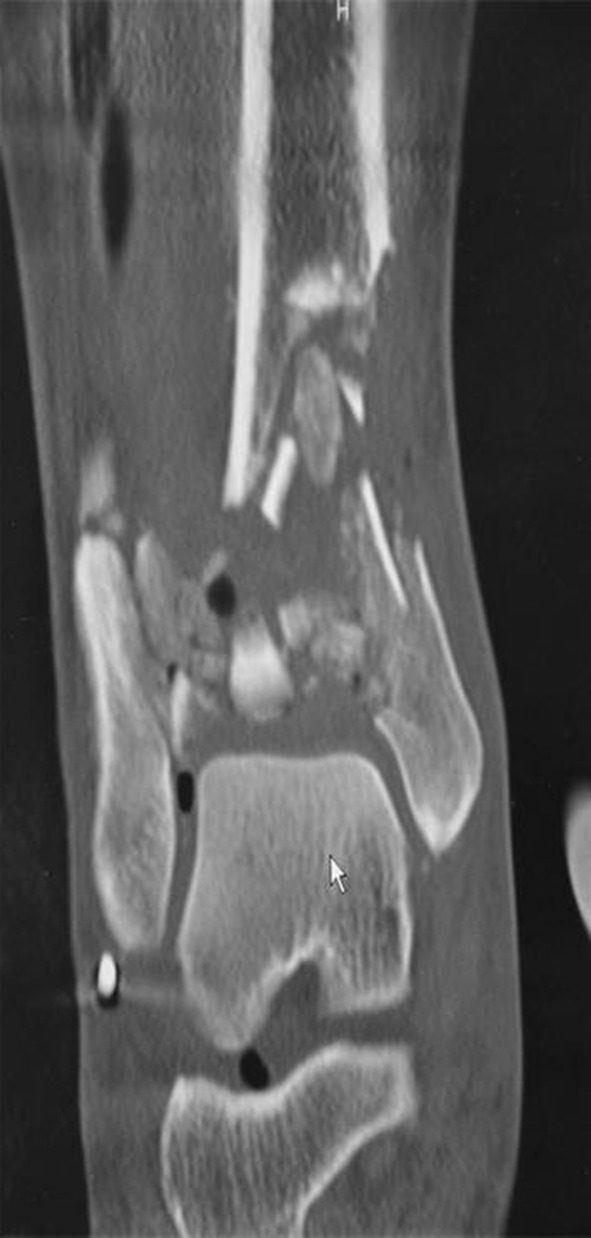
Background: Posttraumatic arthritis and prolonged recovery are typical after a severely comminuted tibial pilon fracture, and ankle arthrodesis is a common salvage procedure. However, few reports discuss the option of immediate arthrodesis, which may be a potentially viable approach to accelerate overall recovery in patients with severe fracture patterns.
Questions/purposes: (1) How long does it take the fracture to heal and the arthrodesis to fuse when primary ankle arthrodesis is a component of initial fracture management? (2) How do these patients fare clinically in terms of modified American Orthopaedic Foot and Ankle Society (AOFAS) scores and activity levels after this treatment? (3) Does primary ankle arthrodesis heal in an acceptable position when anterior ankle arthrodesis plates are used?
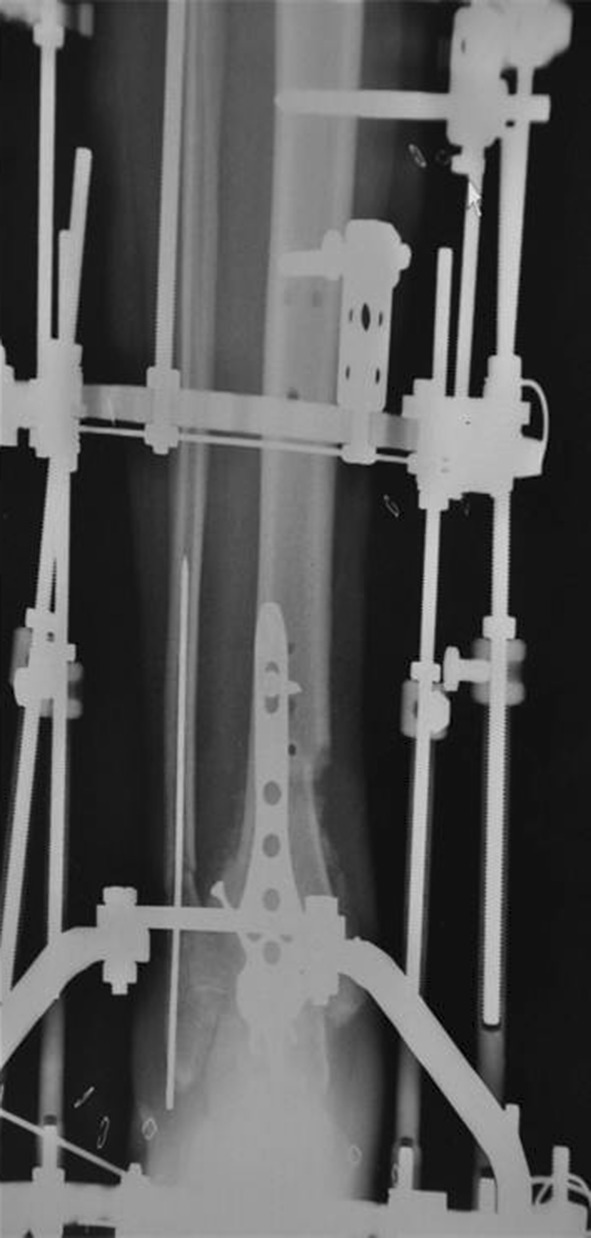
Methods: During a 2-year period, we performed open fracture reduction and internal fixation in 63 patients. Eleven patients (12 ankles) with severely comminuted high-energy tibial pilon fractures were retrospectively reviewed after surgical treatment with primary ankle arthrodesis and fracture reduction. Average patient age was 58 years, and minimum followup was 6 months (average, 14 months; range, 6-22 months). Anatomically designed anterior ankle arthrodesis plates were used in 10 ankles. Ring external fixation was used in nine ankles with concomitant tibia fracture or in instances requiring additional fixation. Clinical evaluation included chart review, interview, the AOFAS ankle-hindfoot score, and radiographic evaluation.
Results: All of the ankle arthrodeses healed at an average of 4.4 months (range, 3-5 months). One patient had a nonunion at the metaphyseal fracture, which healed with revision surgery. The average AOFAS ankle-hindfoot score was 83 with 88% having an excellent or good result. Radiographic and clinical analysis confirmed a plantigrade foot without malalignment. No patients required revision surgery for malunion.
Conclusions: Primary ankle arthrodesis combined with fracture reduction for the severely comminuted tibial pilon fracture reliably healed and restored acceptable function in this highly selective patient group. Ring external fixation may be a useful adjunct to internal fixation, and this concept should be further studied.
Level of evidence: Level IV, therapeutic study. See Guidelines for Authors for a complete description of levels of evidence.
Figures
















References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
