

Non-thyroidal illness in the ICU: a syndrome with different faces
- PMID: 24845024
- PMCID: PMC4195234
- DOI: 10.1089/thy.2014.0201
Non-thyroidal illness in the ICU: a syndrome with different faces
Abstract
Background: Critically ill patients typically present with low or low-normal plasma thyroxine, low plasma triiodothyronine (T3), increased plasma reverse T3 (rT3) concentrations, in the absence of a rise in thyrotropin (TSH). This constellation is referred to as nonthyroidal illness syndrome (NTI). Although it is long known that the severity of NTI is associated with risk of poor outcomes of critical illness, the causality in this association has not been well investigated.
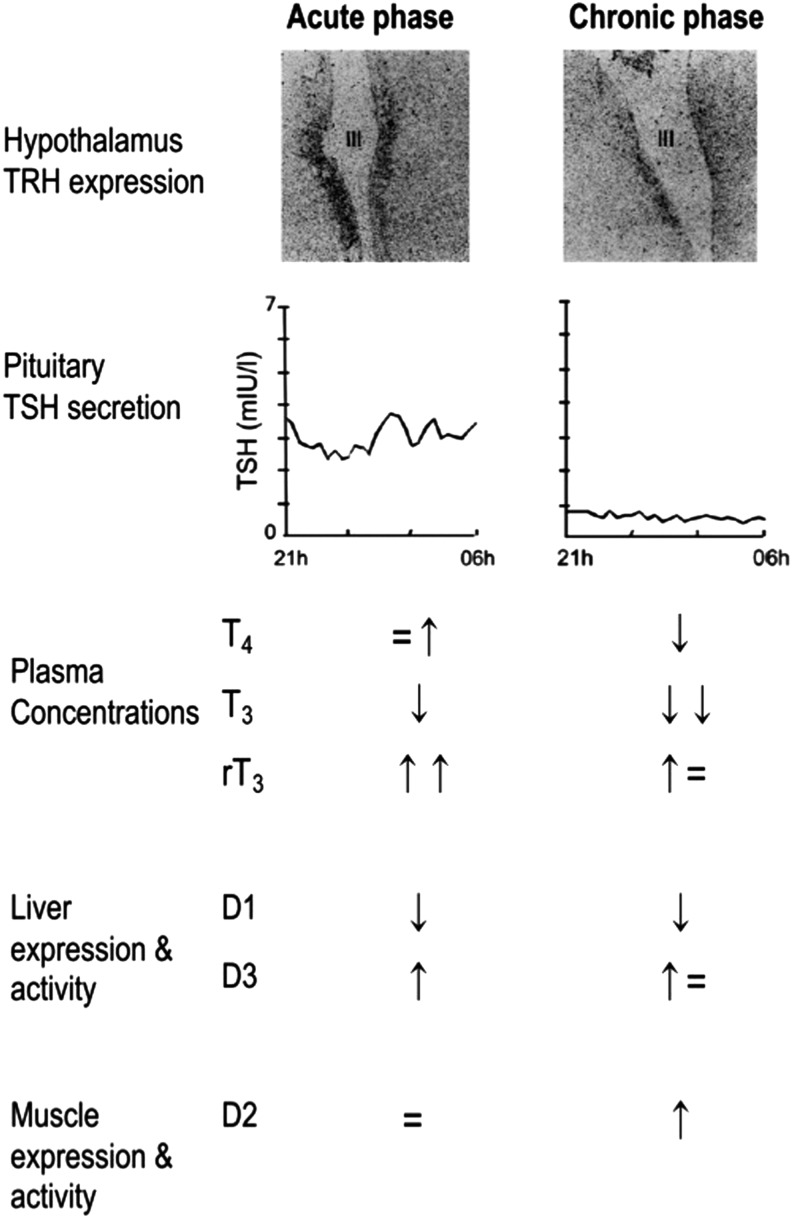
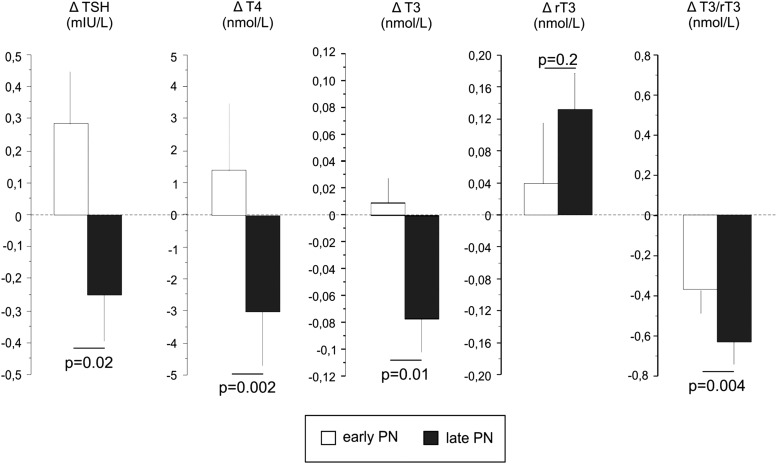
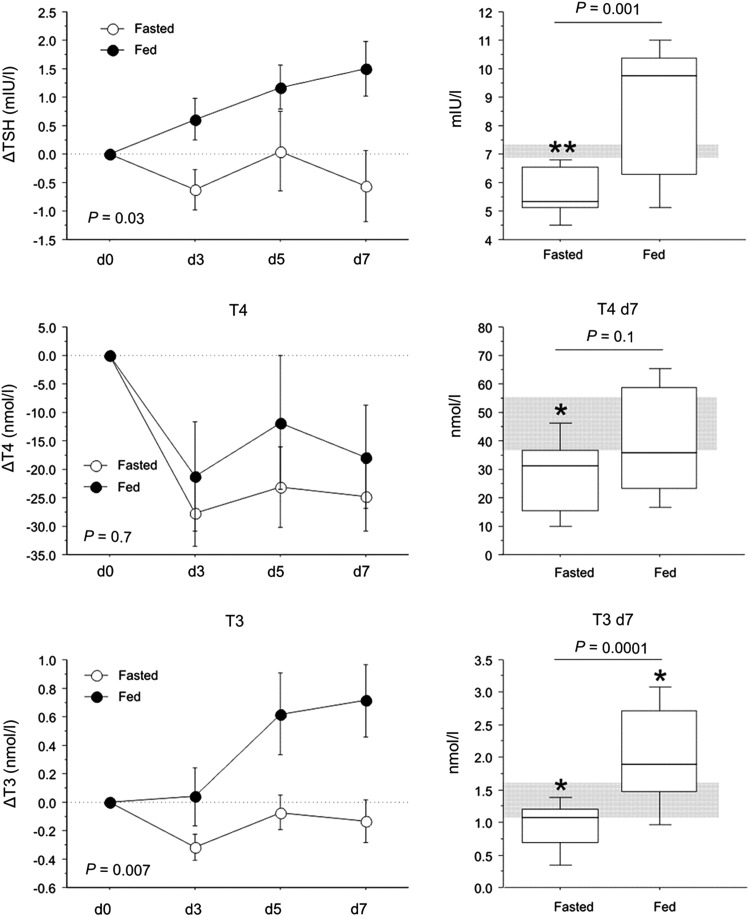
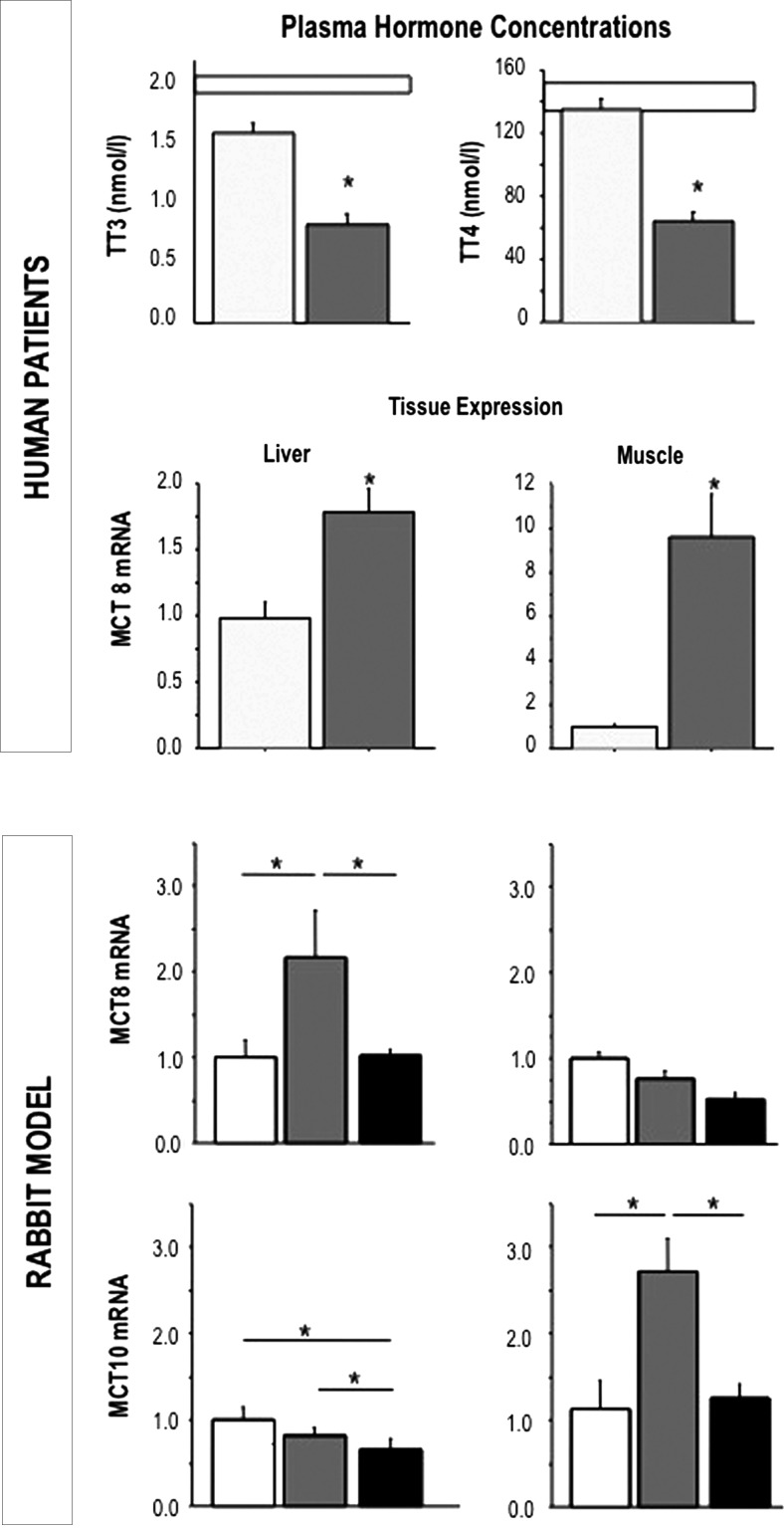
Summary: In this narrative review, the different faces of NTI during critical illness are highlighted. Acute alterations are dominated by changes in thyroid hormone binding, peripheral thyroid hormone uptake, and alterations in the expression and activity of the type-1 and type-3 deiodinases. It was recently shown that at least part of these acute changes are brought about by concomitant macronutrient restriction, and this part appears adaptive and beneficial. However, the face of the NTI in the prolonged phase of critical illness is different, when patients are fully fed but continue to depend on intensive medical care. In that prolonged phase of illness, hypothalamic thyrotropin releasing hormone (TRH) expression is suppressed and explains reduced TSH secretion and whereby reduced thyroidal hormone release. During prolonged critical illness, and in the presence of adequate nutrition, several tissue responses could be interpreted as compensatory to low thyroid hormone availability, such as increased expression of monocarboxylate transporters, upregulation of type-2 deiodinase activity, and increased sensitivity at the receptor level. Infusing hypothalamic releasing factors in these prolonged critically ill patients can reactivate the thyroid axis and induce an anabolic response.
Conclusions: It is clear that the name "NTI" during critical illness refers to a syndrome with different faces. Tolerating the early "fasting response" to critical illness and its concomitant changes in thyroid hormone parameters appears to be wise and beneficial. This thus applies to the NTI present in the majority of the patients treated in intensive care units. However, the NTI that occurs in prolonged critically ill patients appears different with regard to both its causes and consequences. Future studies should specifically target this selected population of prolonged critically ill patients, and, after excluding iatrogic drug interferences, investigate the effect on outcome of treatment with hypothalamic releasing factors in adequately powered randomized controlled trials.
Figures
References
-
- Utiger RD.1980Decreased extrathyroidal triiodothyronine production in nonthyroidal illness: benefit or harm? Am J Med 69:807–810 - PubMed
-
- Wartofsky L, Burman KD.1982Alterations in thyroid function in patients with systemic illness: the “euthyroid sick syndrome.” Endocr Rev 3:164–217 - PubMed
-
- Van den Berghe G, de Zegher F, Bouillon R.1998Acute and prolonged critical illness as different neuroendocrine paradigms. J Clin Endocrinol Metab 83:1827–1834 - PubMed
-
- Boelen A, Kwakkel J, Fliers E.2011Beyond low plasma T3: local thyroid hormone metabolism during inflammation and infection. Endocr Rev 32:670–693 - PubMed
-
- Boonen E, Van den Berghe G.2014Endocrine responses to critical illness: novel insights and therapeutic implications. J Clin Endocrinol Metab 99:1569–1582 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
