

A prospective study comparing the predictions of doctors versus models for treatment outcome of lung cancer patients: a step toward individualized care and shared decision making
- PMID: 24846083
- PMCID: PMC4886657
- DOI: 10.1016/j.radonc.2014.04.012
A prospective study comparing the predictions of doctors versus models for treatment outcome of lung cancer patients: a step toward individualized care and shared decision making
Abstract
Background: Decision Support Systems, based on statistical prediction models, have the potential to change the way medicine is being practiced, but their application is currently hampered by the astonishing lack of impact studies. Showing the theoretical benefit of using these models could stimulate conductance of such studies. In addition, it would pave the way for developing more advanced models, based on genomics, proteomics and imaging information, to further improve the performance of the models.
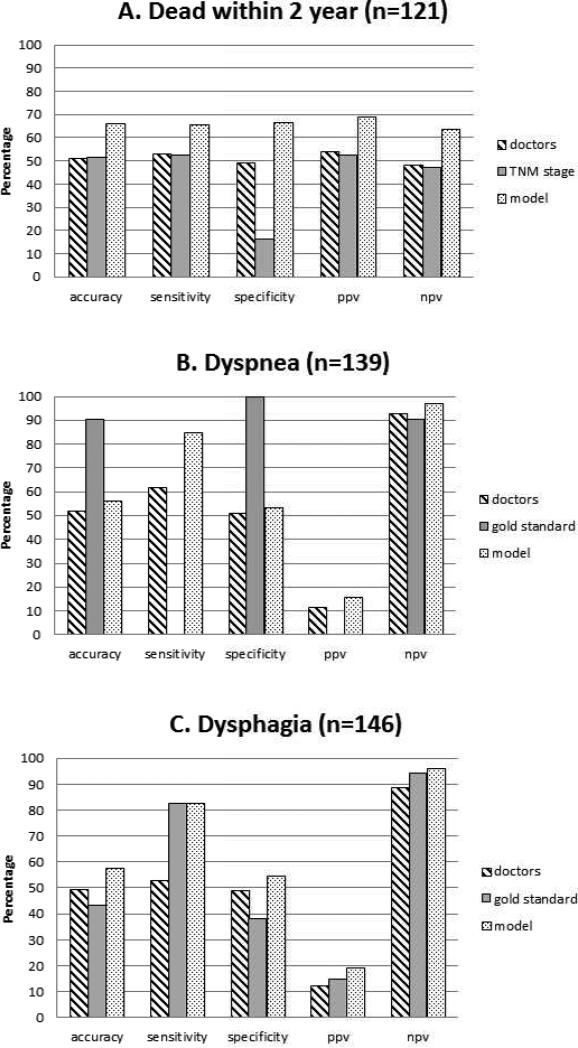
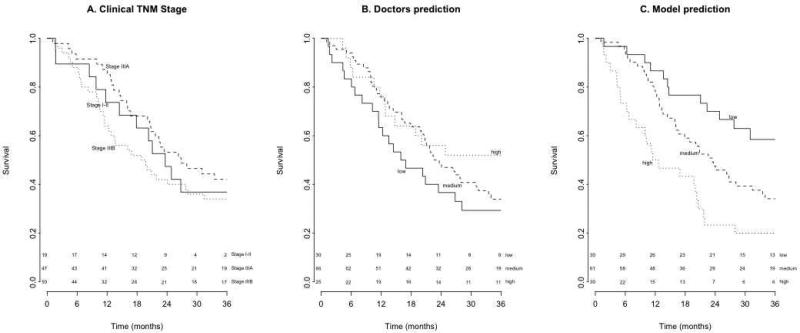
Purpose: In this prospective single-center study, previously developed and validated statistical models were used to predict the two-year survival (2yrS), dyspnea (DPN), and dysphagia (DPH) outcomes for lung cancer patients treated with chemo radiation. These predictions were compared to probabilities provided by doctors and guideline-based recommendations currently used. We hypothesized that model predictions would significantly outperform predictions from doctors.
Materials and methods: Experienced radiation oncologists (ROs) predicted all outcomes at two timepoints: (1) after the first consultation of the patient, and (2) after the radiation treatment plan was made. Differences in the performances of doctors and models were assessed using Area Under the Curve (AUC) analysis.
Results: A total number of 155 patients were included. At timepoint #1 the differences in AUCs between the ROs and the models were 0.15, 0.17, and 0.20 (for 2yrS, DPN, and DPH, respectively), with p-values of 0.02, 0.07, and 0.03. Comparable differences at timepoint #2 were not statistically significant due to the limited number of patients. Comparison to guideline-based recommendations also favored the models.
Conclusion: The models substantially outperformed ROs' predictions and guideline-based recommendations currently used in clinical practice. Identification of risk groups on the basis of the models facilitates individualized treatment, and should be further investigated in clinical impact studies.
Keywords: Lung cancer; Prediction models.
Copyright © 2014 Elsevier Ireland Ltd. All rights reserved.
Figures
References
-
- Dehing-Oberije C, Yu S, De Ruysscher D, Meersschout S, Van Beek K, Lievens Y, et al. Development and external validation of prognostic model for 2-year survival of non-small-cell lung cancer patients treated with chemoradiotherapy. Int J Radiat Oncol Biol Phys. 2009;74:355–62. - PubMed
-
- Dehing-Oberije C, De Ruysscher D, Petit S, Van Meerbeeck J, Vandecasteele K, De Neve W, et al. Development, external validation and clinical usefulness of a practical prediction model for radiation-induced dysphagia in lung cancer patients. Radiother Oncol. 2010;97:455–61. - PubMed
-
- Dehing-Oberije C, De Ruysscher D, van Baardwijk A, Yu S, Rao B, Lambin P. The importance of patient characteristics for the prediction of radiation-induced lung toxicity. Radiother Oncol. 2009;91:421–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
