

Time to administration of epinephrine and outcome after in-hospital cardiac arrest with non-shockable rhythms: retrospective analysis of large in-hospital data registry
- PMID: 24846323
- PMCID: PMC4027796
- DOI: 10.1136/bmj.g3028
Time to administration of epinephrine and outcome after in-hospital cardiac arrest with non-shockable rhythms: retrospective analysis of large in-hospital data registry
Abstract
Objective: To determine if earlier administration of epinephrine (adrenaline) in patients with non-shockable cardiac arrest rhythms is associated with increased return of spontaneous circulation, survival, and neurologically intact survival.
Design: Post hoc analysis of prospectively collected data in a large multicenter registry of in-hospital cardiac arrests (Get With The Guidelines-Resuscitation).
Setting: We utilized the Get With The Guidelines-Resuscitation database (formerly National Registry of Cardiopulmonary Resuscitation, NRCPR). The database is sponsored by the American Heart Association (AHA) and contains prospective data from 570 American hospitals collected from 1 January 2000 to 19 November 2009.
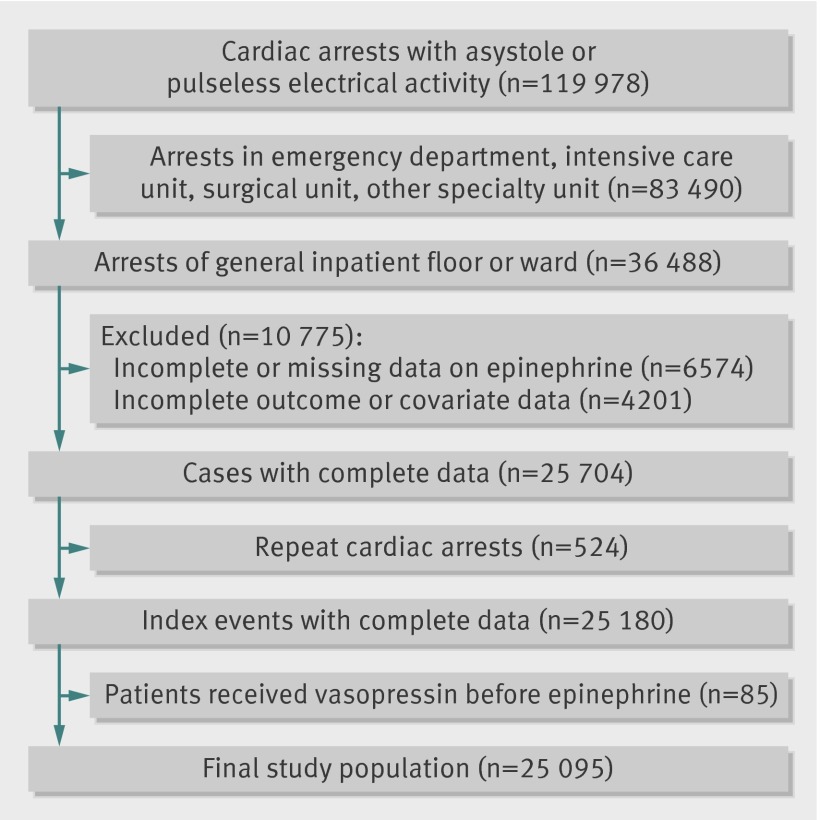
Participants: 119,978 adults from 570 hospitals who had a cardiac arrest in hospital with asystole (55%) or pulseless electrical activity (45%) as the initial rhythm. Of these, 83,490 arrests were excluded because they took place in the emergency department, intensive care unit, or surgical or other specialty unit, 10,775 patients were excluded because of missing or incomplete data, 524 patients were excluded because they had a repeat cardiac arrest, and 85 patients were excluded as they received vasopressin before the first dose of epinephrine. The main study population therefore comprised 25,095 patients. The mean age was 72, and 57% were men.
Main outcome measures: The primary outcome was survival to hospital discharge. Secondary outcomes included sustained return of spontaneous circulation, 24 hour survival, and survival with favorable neurologic status at hospital discharge.
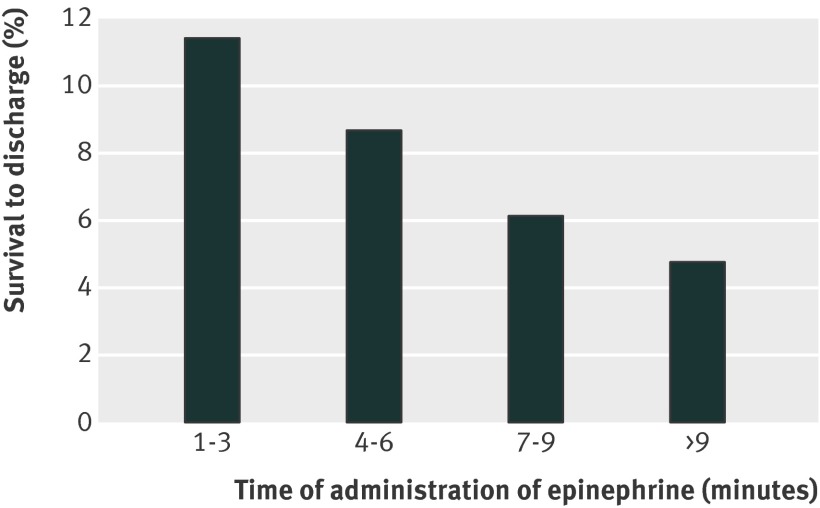
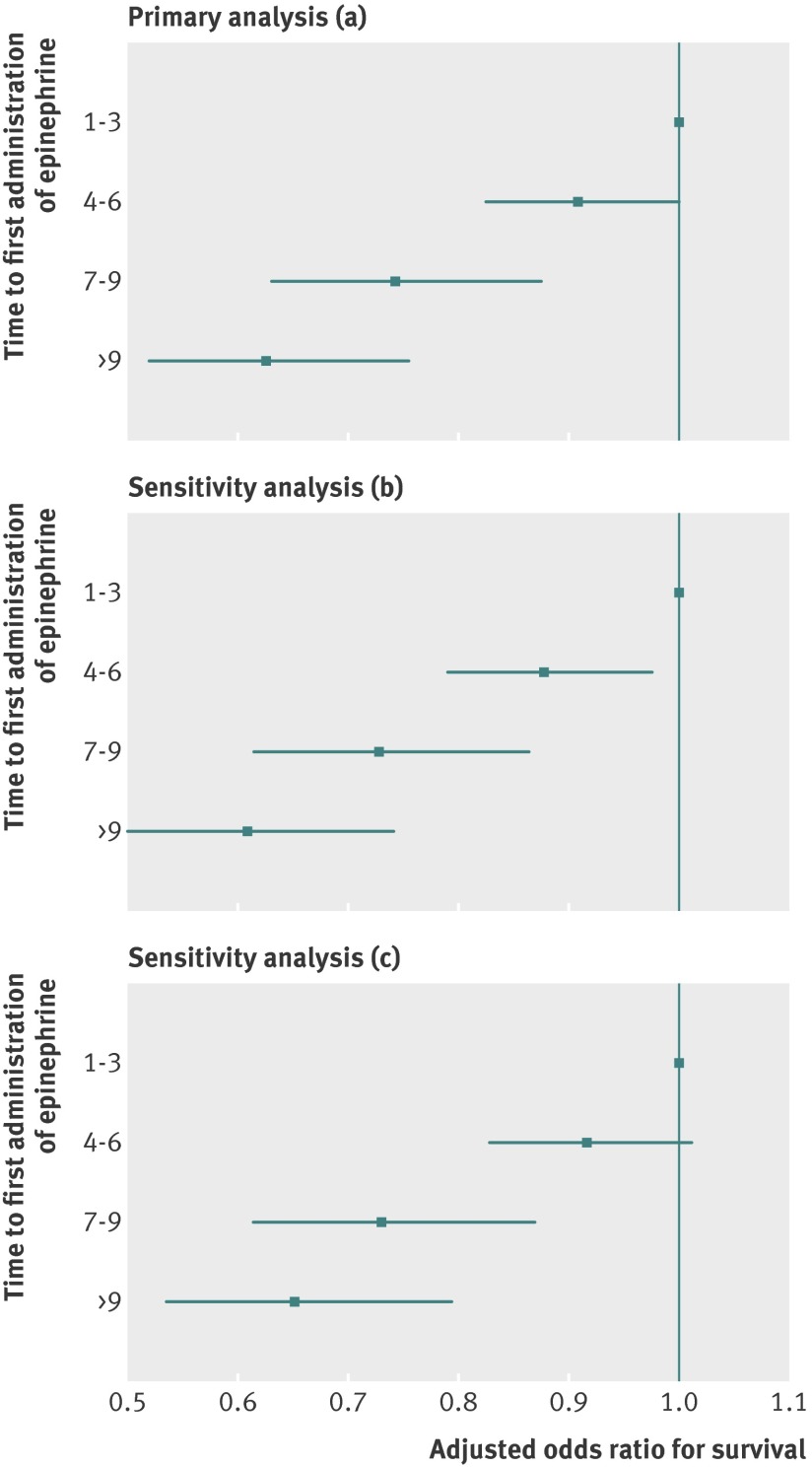
Results: 25,095 adults had in-hospital cardiac arrest with non-shockable rhythms. Median time to administration of the first dose of epinephrine was 3 minutes (interquartile range 1-5 minutes). There was a stepwise decrease in survival with increasing interval of time to epinephrine (analyzed by three minute intervals): adjusted odds ratio 1.0 for 1-3 minutes (reference group); 0.91 (95% confidence interval 0.82 to 1.00; P=0.055) for 4-6 minutes; 0.74 (0.63 to 0.88; P<0.001) for 7-9 minutes; and 0.63 (0.52 to 0.76; P<0.001) for >9 minutes. A similar stepwise effect was observed across all outcome variables.
Conclusions: In patients with non-shockable cardiac arrest in hospital, earlier administration of epinephrine is associated with a higher probability of return of spontaneous circulation, survival in hospital, and neurologically intact survival.
© Donnino et al 2014.
Conflict of interest statement
Competing interest: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Early adrenaline for cardiac arrest.BMJ. 2014 May 29;348:g3245. doi: 10.1136/bmj.g3245. BMJ. 2014. PMID: 24874448 No abstract available.
References
-
- Bedell SE, Delbanco TL, Cook EF, Epstein FH. Survival after cardiopulmonary resuscitation in the hospital. N Engl J Med 1983;309:569-76. - PubMed
-
- Nadkarni VM, Larkin GL, Peberdy MA, Carey SM, Kaye W, Mancini ME, et al. First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults. JAMA 2006;295:50. - PubMed
-
- Peberdy MA, Kaye W, Ornato JP, Larkin GL, Nadkarni V, Mancini ME, et al. Cardiopulmonary resuscitation of adults in the hospital: a report of 14 720 cardiac arrests from the National Registry of Cardiopulmonary Resuscitation. Resuscitation 2003;58:297-308. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical