

Mortality among tuberculosis patients with acquired resistance to second-line antituberculosis drugs--United States, 1993-2008
- PMID: 24846639
- PMCID: PMC4784225
- DOI: 10.1093/cid/ciu372
Mortality among tuberculosis patients with acquired resistance to second-line antituberculosis drugs--United States, 1993-2008
Abstract
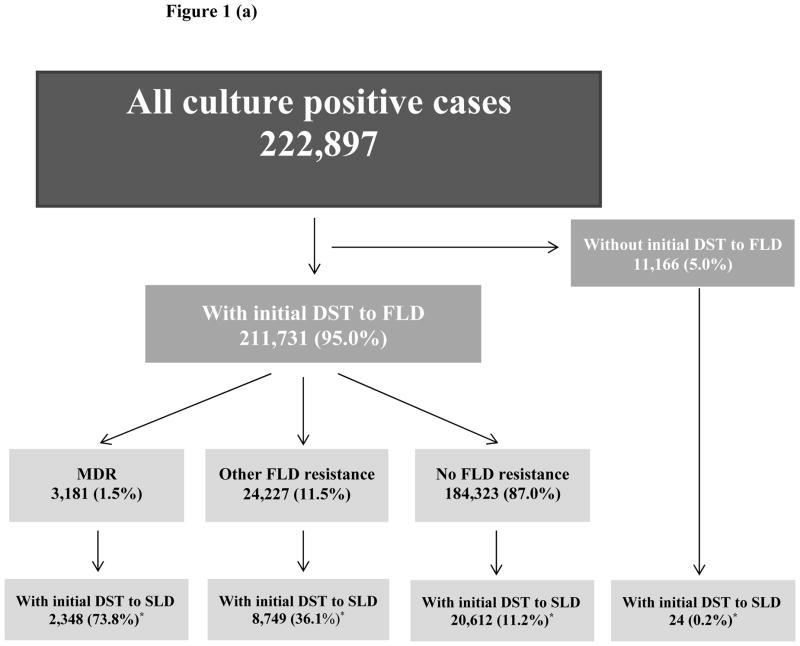
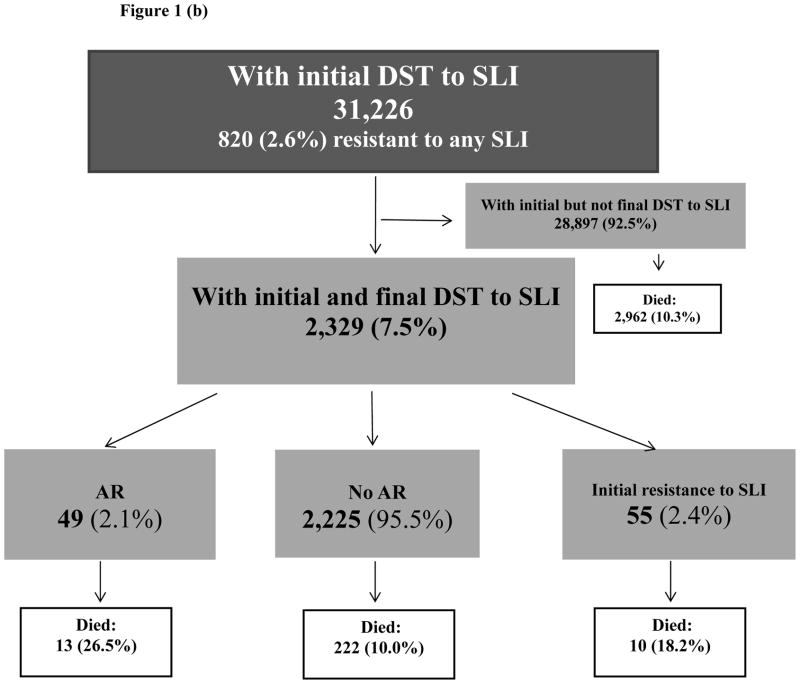
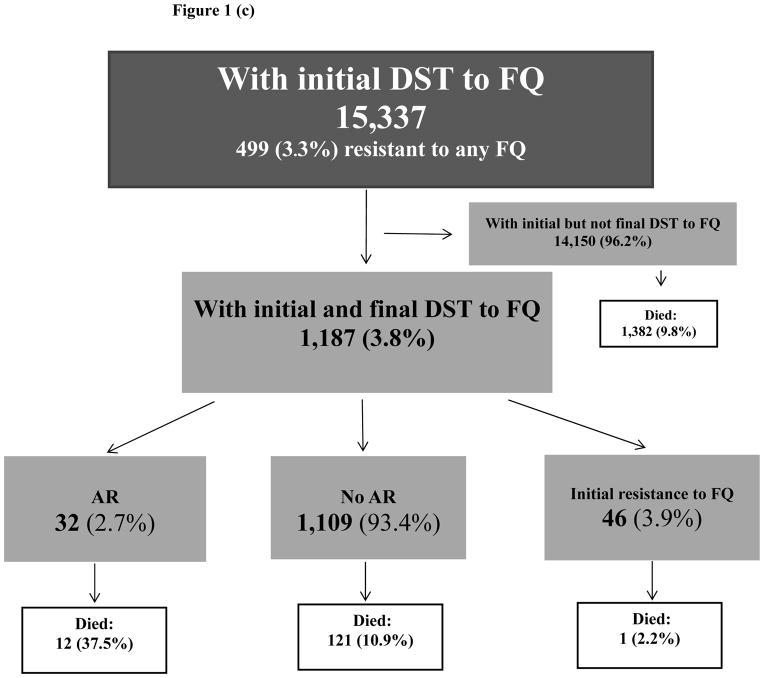
Background: Resistance to second-line antituberculosis drugs (SLDs) severely compromises treatment options of drug-resistant tuberculosis. We assessed the association between acquisition of resistance (AR) to second-line injectable drugs (SLIs) or fluoroquinolones (FQs) and mortality among tuberculosis cases confirmed by positive culture results with available initial and final drug susceptibility test (DST) results.
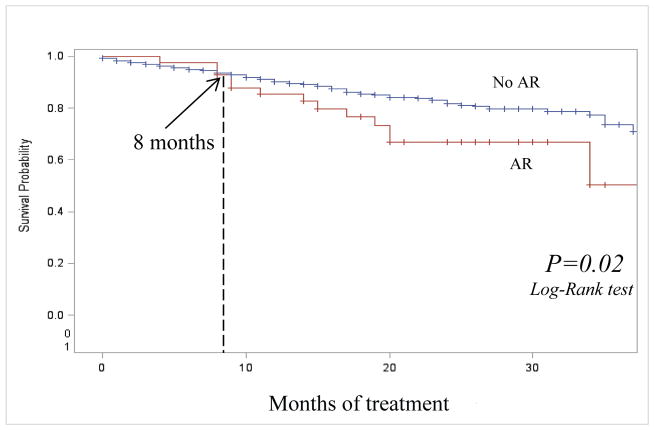
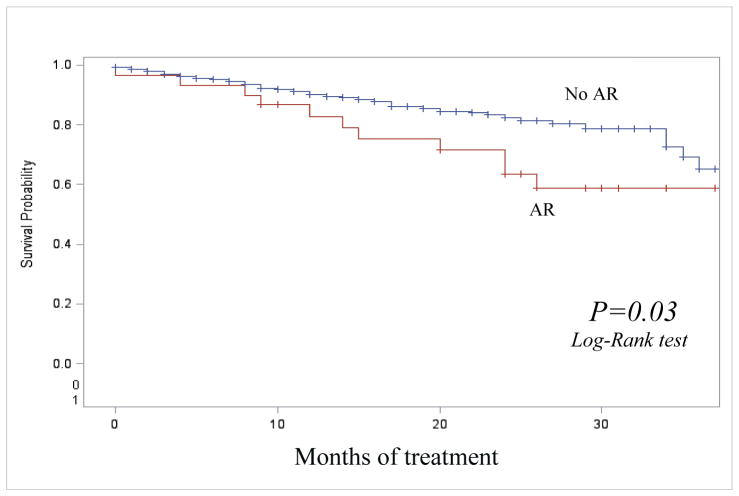
Methods: We analyzed data from the US National Tuberculosis Surveillance System, 1993-2008. Acquired resistance was defined as drug susceptibility at initial DST but resistance to the same drug at final DST. We compared survival with Kaplan-Meier curves and analyzed the association between AR and mortality using a univariate extended Cox proportional hazards model adjusted for age.
Results: Of 2329 cases with both initial and final DSTs to SLIs, 49 (2.1%) acquired resistance; 13 of 49 (26.5%) had treatment terminated by death compared with 222 (10.0%) of those without AR to SLIs (P < .001). Of 1187 cases with both initial and final DSTs to FQs, 32 (2.8%) acquired resistance; 12 of 32 (37.5%) had treatment terminated by death compared with 121 (10.9%) of those without AR to FQs (P = .001). Controlling for age, mortality was significantly greater among cases with AR to SLDs than among cases without AR (adjusted hazard ratio [aHR] for SLIs: 2.8; 95% confidence interval [CI],1.4-5.4; aHR for FQ: 1.9; 95% CI, 1.0-3.5). Multidrug-resistant tuberculosis at treatment initiation, positive human immunodeficiency virus status, and extrapulmonary disease were also significantly associated with mortality.
Conclusions: Mortality was significantly greater among tuberculosis cases with AR to SLDs. Providers should consider AR to SLDs early in treatment, monitor DST results, and avoid premature deaths.
Keywords: acquired drug resistance; tuberculosis.
Published by Oxford University Press on behalf of the Infectious Diseases Society of America 2014. This work is written by (a) US Government employee(s) and is in the public domain in the US.
Figures
Similar articles
-
Acquired resistance to second-line drugs among persons with tuberculosis in the United States.Clin Infect Dis. 2012 Dec;55(12):1600-7. doi: 10.1093/cid/cis748. Epub 2012 Aug 31. Clin Infect Dis. 2012. PMID: 22942206 Free PMC article.
-
Resistance to Second-Line Antituberculosis Drugs and Delay in Drug Susceptibility Testing among Multidrug-Resistant Tuberculosis Patients in Shanghai.Biomed Res Int. 2016;2016:2628913. doi: 10.1155/2016/2628913. Epub 2016 Aug 29. Biomed Res Int. 2016. PMID: 27652260 Free PMC article.
-
Extensive drug resistance acquired during treatment of multidrug-resistant tuberculosis.Clin Infect Dis. 2014 Oct 15;59(8):1049-63. doi: 10.1093/cid/ciu572. Epub 2014 Jul 23. Clin Infect Dis. 2014. PMID: 25057101 Free PMC article.
-
High degree of fluoroquinolone resistance among extrapulmonary tuberculosis patients at a tertiary care center in North India.Int J Mycobacteriol. 2020 Jul-Sep;9(3):309-312. doi: 10.4103/ijmy.ijmy_116_20. Int J Mycobacteriol. 2020. PMID: 32862166
-
Current prospects for the fluoroquinolones as first-line tuberculosis therapy.Antimicrob Agents Chemother. 2011 Dec;55(12):5421-9. doi: 10.1128/AAC.00695-11. Epub 2011 Aug 29. Antimicrob Agents Chemother. 2011. PMID: 21876059 Free PMC article. Review.
Cited by
-
Acquired Resistance to Antituberculosis Drugs in England, Wales, and Northern Ireland, 2000-2015.Emerg Infect Dis. 2018 Mar;24(3):524-533. doi: 10.3201/eid2403.171362. Emerg Infect Dis. 2018. PMID: 29460735 Free PMC article.
-
Transmission is a Noticeable Cause of Resistance Among Treated Tuberculosis Patients in Shanghai, China.Sci Rep. 2017 Aug 9;7(1):7691. doi: 10.1038/s41598-017-08061-3. Sci Rep. 2017. PMID: 28794425 Free PMC article.
-
Multidrug-Resistant Tuberculosis Treatment Outcomes in Relation to Treatment and Initial Versus Acquired Second-Line Drug Resistance.Clin Infect Dis. 2016 Feb 15;62(4):418-430. doi: 10.1093/cid/civ910. Epub 2015 Oct 27. Clin Infect Dis. 2016. PMID: 26508515 Free PMC article.
-
Estimating the burden of antimicrobial resistance: a systematic literature review.Antimicrob Resist Infect Control. 2018 Apr 25;7:58. doi: 10.1186/s13756-018-0336-y. eCollection 2018. Antimicrob Resist Infect Control. 2018. PMID: 29713465 Free PMC article.
References
-
- World Health Organization. Global Tuberculosis Control 2013. Geneva, Switzerland: WHO; 2013. Available at http://www.who.int/tb/publications/global_report/en/
-
- Caminero J. Multidrug-resistant tuberculosis: epidemiology, risk factors and case finding. Int J Tuberc Lung Dis. 2010 Apr;14(4):382–90. - PubMed
-
- Monedero I, Caminero J. Management of multidrug-resistant tuberculosis: an update. Ther Adv Respir Dis. 2010 Apr;4(2):117–27. - PubMed
-
- World Health Organization. The Global Plan to Stop TB 2011–2015. Geneva, Switzerland: WHO; 2010. Available at http://www.stoptb.org/assets/documents/global/plan/TB_GlobalPlanToStopTB....
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
