

Atherogenesis and iron: from epidemiology to cellular level
- PMID: 24847266
- PMCID: PMC4017151
- DOI: 10.3389/fphar.2014.00094
Atherogenesis and iron: from epidemiology to cellular level
Abstract
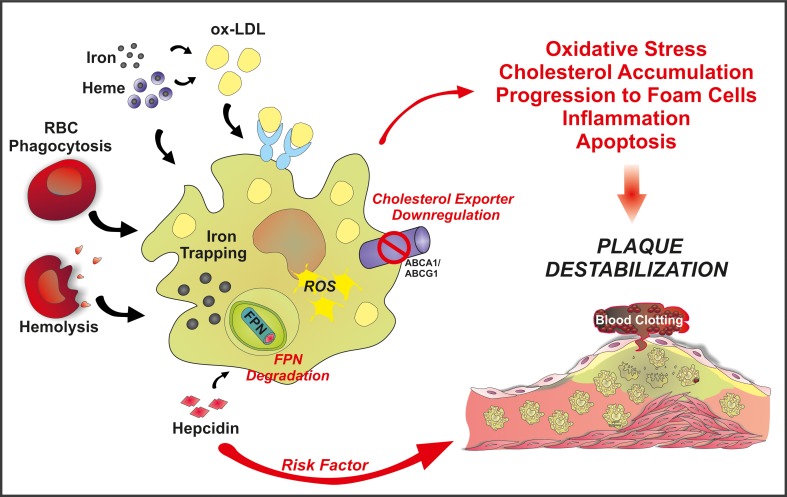
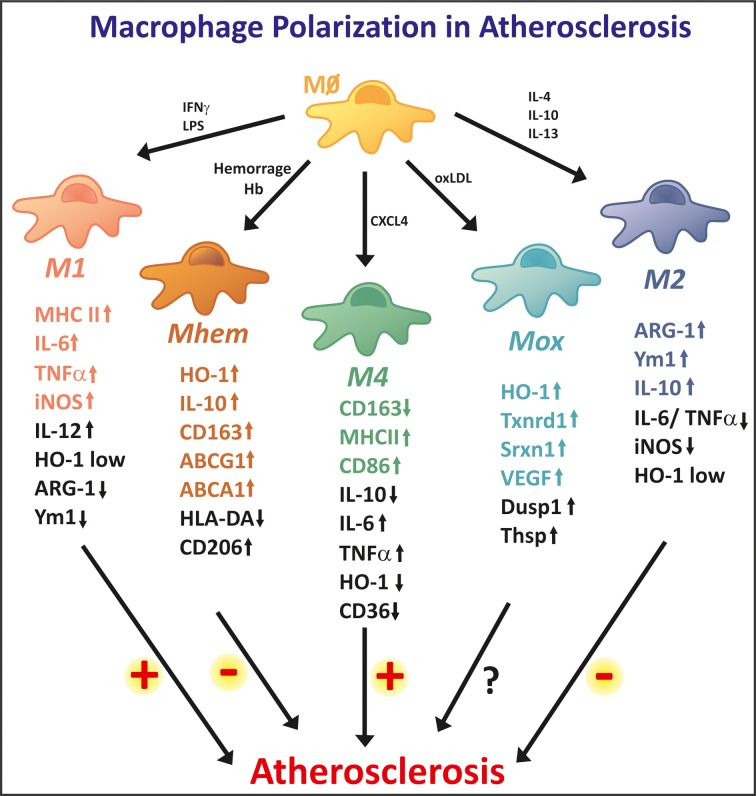
Iron accumulates in human atherosclerotic lesions but whether it is a cause or simply a downstream consequence of the atheroma formation has been an open question for decades. According to the so called "iron hypothesis," iron is believed to be detrimental for the cardiovascular system, thus promoting atherosclerosis development and progression. Iron, in its catalytically active form, can participate in the generation of reactive oxygen species and induce lipid-peroxidation, triggering endothelial activation, smooth muscle cell proliferation and macrophage activation; all of these processes are considered to be proatherogenic. On the other hand, the observation that hemochromatotic patients, affected by life-long iron overload, do not show any increased incidence of atherosclerosis is perceived as the most convincing evidence against the "iron hypothesis." Epidemiological studies and data from animal models provided conflicting evidences about the role of iron in atherogenesis. Therefore, more careful studies are needed in which issues like the source and the compartmentalization of iron will be addressed. This review article summarizes what we have learnt about iron and atherosclerosis from epidemiological studies, animal models and cellular systems and highlights the rather contributory than innocent role of iron in atherogenesis.
Keywords: LDL; atherosclerosis; heme; hemoglobin; intraplaque hemorrhage; iron; macrophages; oxidative stress.
Figures

References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources