

Iodine Supplementation throughout Pregnancy Does Not Prevent the Drop in FT4 in the Second and Third Trimesters in Women with Normal Initial Thyroid Function
- PMID: 24847452
- PMCID: PMC4017760
- DOI: 10.1159/000350882
Iodine Supplementation throughout Pregnancy Does Not Prevent the Drop in FT4 in the Second and Third Trimesters in Women with Normal Initial Thyroid Function
Abstract
Objectives: The aim of the study was to determine the evolution of thyroid tests throughout pregnancy and postpartum in healthy women with and without iodine supplementation.
Methods: This was a prospective, randomized, interventional study of iodine supplementation (150 μg/day) from the first trimester until 3 months postpartum versus controls. 111 pregnant women with normal initial thyroid tests were enrolled, undergoing comprehensive thyroid assessment at each trimester. We present results of longitudinal and cross-sectional analyses.
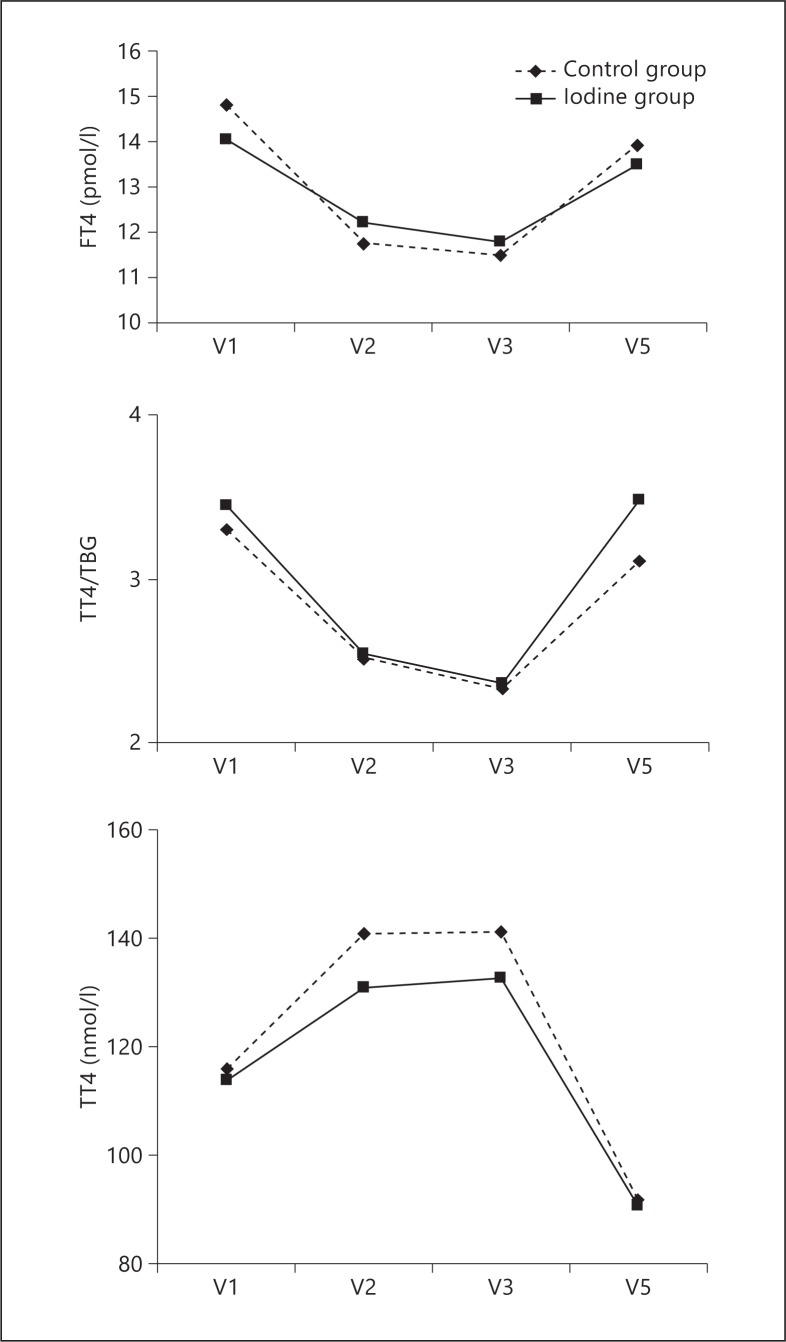
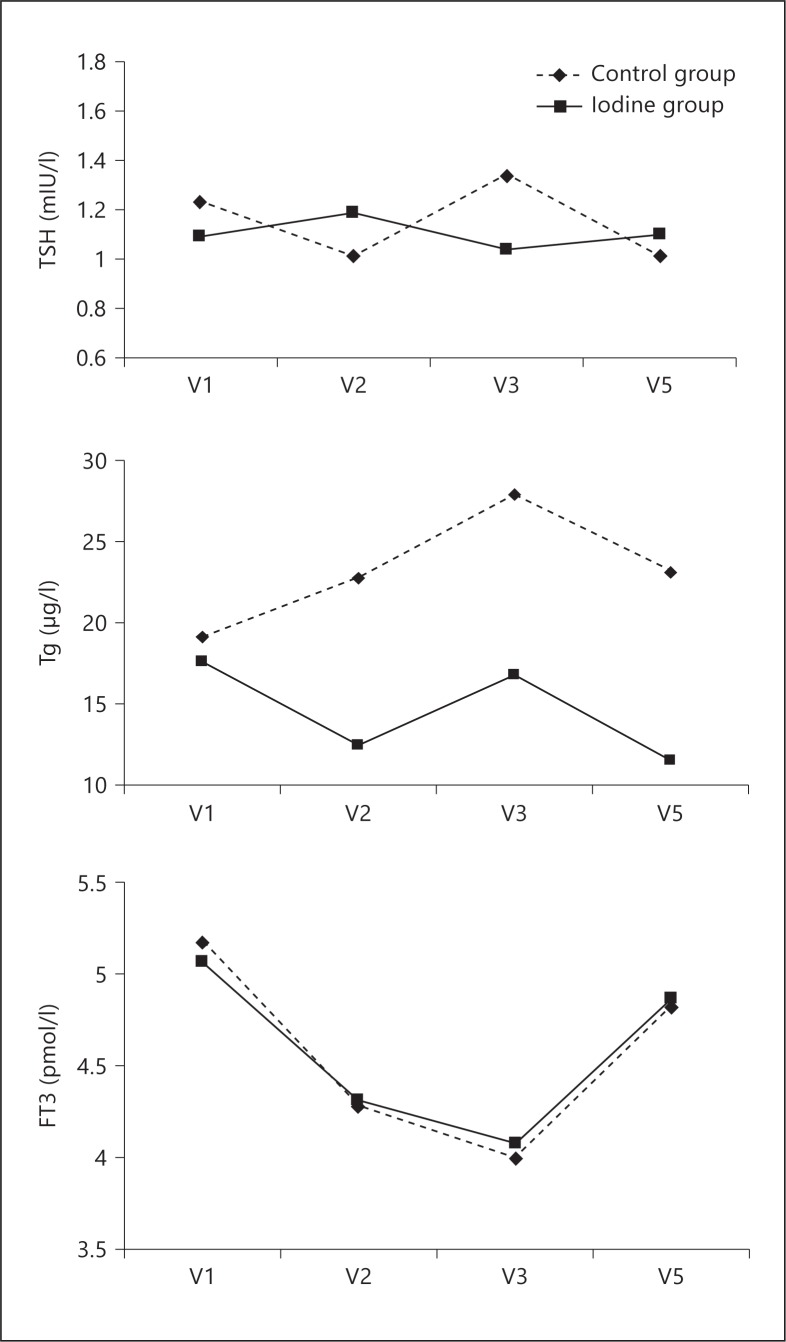
Results: Initial ioduria suggested mild iodine deficiency in both groups, while third-trimester ioduria rose to levels of iodine sufficiency in the iodine-supplemented group. In the longitudinal study, free T4 (FT4) levels decreased in the second and third trimesters compared to the first trimester in both groups, with no change in TSH, and rose postpartum, though lower than the first trimester. FT3 levels and the total T4 (TT4)/thyroxine-binding globulin (TBG) ratio followed the same evolution as FT4. TT4 levels rose due to TBG increase. Thyroglobulin (Tg) of iodine group remained stable, contrasting with the rise in the control group. In the cross-sectional study, there was no difference between the two groups in thyroid tests at any time-point, except for lower Tg in the second trimester and postpartum visits in the iodine group.
Conclusions: In healthy, mildly iodine-deficient pregnant women, a 'drop' of FT4 and TT4/TBG without TSH increase occurs between the first and second trimesters, and is not prevented by iodine supplementation, suggesting physiology. Therefore, FT4 is valuable to assess thyroid function in pregnancy in clinical practice with appropriate trimester-specific reference range. It brings up reflection on threshold for diagnosis and treatment of hypothyroxinemia.
Keywords: Free T4; Iodine; Ioduria; Pregnancy; Thyroglobulin.
Figures
References
-
- Glinoer D. The regulation of thyroid function in pregnancy: pathways of endocrine adaptation from physiology to pathology. Endocr Rev. 1997;18:404–433. - PubMed
-
- Morreale de Escobar G, Obregon MJ, Escobar del Rey F. Is neuropsychological development related to maternal hypothyroidism or to maternal hypothyroxinemia? J Clin Endocrinol Metab. 2000;85:3975–3987. - PubMed
-
- De Groot L, Abalovich M, Alexander EK, Amino N, Barbour L, Cobin RH, Eastman CJ, Lazarus JH, Luton D, Mandel SJ, Mestman J, Rovet J, Sullivan S. Management of thyroid dysfunction during pregnancy and postpartum: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2012;97:2543–2535. - PubMed
-
- Pop VJ, Brouwers EP, Vader HL, Vulsma T, van Baar AL, de Vijlder JJ. Maternal hypothyroxinaemia during early pregnancy and subsequent child development: a 3 year prospective study. Clin Endocrinol. 2003;59:282–288. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
