

A normal reference of bone mineral density (BMD) measured by dual energy X-ray absorptiometry in healthy thai children and adolescents aged 5-18 years: a new reference for Southeast Asian Populations
- PMID: 24847716
- PMCID: PMC4029563
- DOI: 10.1371/journal.pone.0097218
A normal reference of bone mineral density (BMD) measured by dual energy X-ray absorptiometry in healthy thai children and adolescents aged 5-18 years: a new reference for Southeast Asian Populations
Abstract
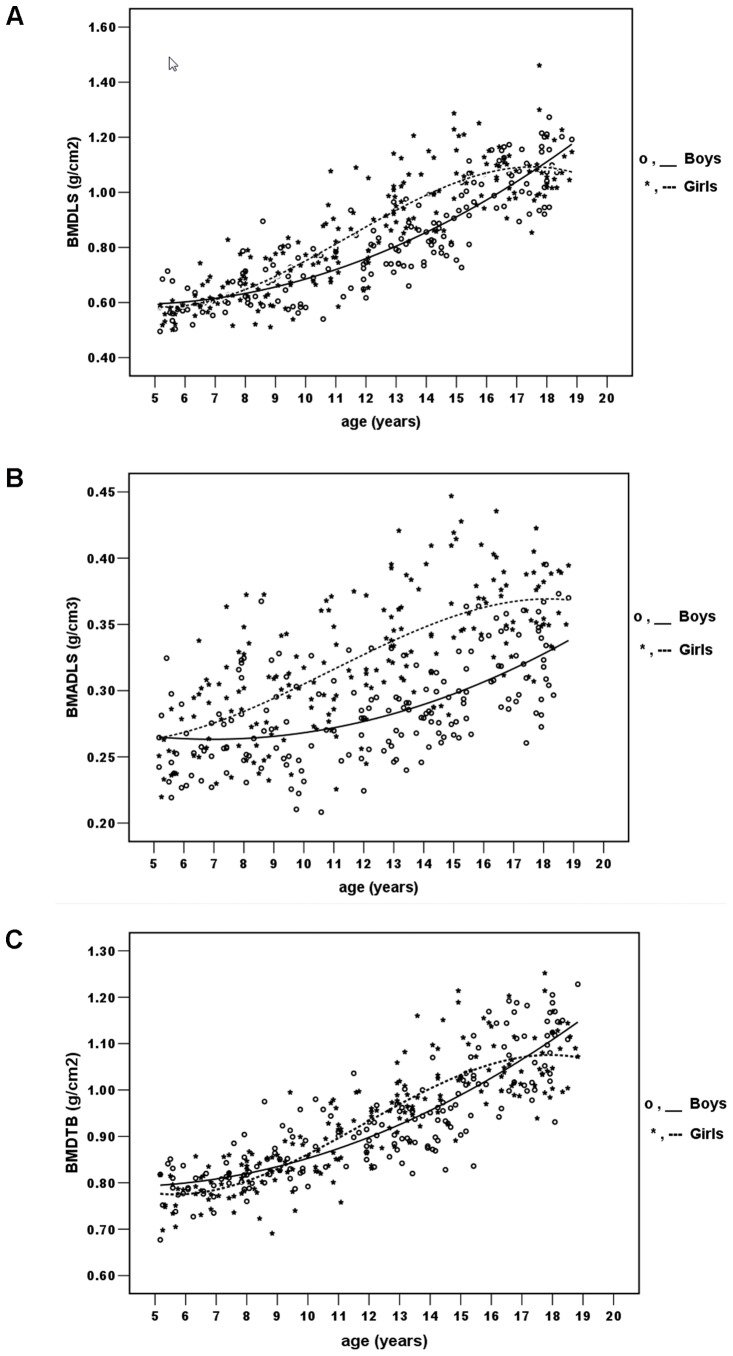
Ethnic-specific normative data of bone mineral density (BMD) is essential for the accurate interpretation of BMD measurement. There have been previous reports of normative BMD data for Caucasian and Asian children including Japanese, Chinese, Korean and Indian. However, the normative BMD data for Southeast Asian including Thai children and adolescents are not currently available. The goals of our study were 1) to establish normative data of BMD, bone mineral content (BMC), bone area (BA) and lean body mass (LBM) for healthy Thai children and adolescents; aged 5-18 years measured by dual energy X-ray absorptiometry (DXA, Lunar Prodigy) and 2) to evaluate the relationships between BMD vs. age, sex, puberty, weight, height, calcium intake and the age of menarche in our population. Gender and age-specific BMD (L2-4; LS and total body; TB), BMADLS (apparent BMD of the lumbar spine), BMC (L2-4 and total body), BA (L2-4 and total body) and LBM were evaluated in 367 children (174 boys and 193 girls). All parameters increased progressively with age. A rapid increase in BMD, BMC and BMADLS was observed at earlier ages in girls. Gender and Tanner stage-specific BMD normative data were also generated. The dynamic changes of BMD values from childhood to early and late puberty of Thai children appeared to be consistent with those of Caucasian and Asian populations. Using a multiple-regression, weight and Tanner stage significantly affected BMDLS, BMDTB and BMADLS in both genders. Only in girls, height was found to have significant influence on BMDTB and BMADLS. The positive correlation between BMD and several demographic parameters, except the calcium intake, was observed. In summary, we established a normal BMD reference for Thai children and adolescents and this will be of useful for clinicians and researchers to appropriately assess BMD in Thais and other Southeast Asian children.
Conflict of interest statement
Figures



Similar articles
-
Updated reference values for BMD and lean mass measured by DXA in Thai children.J Bone Miner Metab. 2024 Nov;42(6):728-740. doi: 10.1007/s00774-024-01550-2. Epub 2024 Sep 13. J Bone Miner Metab. 2024. PMID: 39269509
-
Reference values of bone mineral density of proximal femur for Southeast Asian children and adolescents.Arch Osteoporos. 2022 Nov 19;17(1):145. doi: 10.1007/s11657-022-01184-9. Arch Osteoporos. 2022. PMID: 36400873
-
Bone mineral density by age, gender, pubertal stages, and socioeconomic status in healthy Lebanese children and adolescents.Bone. 2004 Nov;35(5):1169-79. doi: 10.1016/j.bone.2004.06.015. Bone. 2004. PMID: 15542043
-
A Scoping Review of the Recent Clinical Practice Regarding the Evaluation of Bone Mineral Density in Children and Adolescents with Neuromuscular Diseases.Medicina (Kaunas). 2023 Feb 8;59(2):312. doi: 10.3390/medicina59020312. Medicina (Kaunas). 2023. PMID: 36837513 Free PMC article.
-
Effect of breastfeeding on bone mass from childhood to adulthood: a systematic review of the literature.Int Breastfeed J. 2015 Nov 20;10:31. doi: 10.1186/s13006-015-0056-3. eCollection 2015. Int Breastfeed J. 2015. PMID: 26594232 Free PMC article. Review.
Cited by
-
Sex differences in the relationship between body composition and biomarkers of bone and fat metabolism in obese boys and girls.Bone Rep. 2021 May 4;14:101087. doi: 10.1016/j.bonr.2021.101087. eCollection 2021 Jun. Bone Rep. 2021. PMID: 34026951 Free PMC article.
-
Pediatric data for dual X-ray absorptiometric measures of normal lumbar bone mineral density in children under 5 years of age using the lunar prodigy densitometer.J Musculoskelet Neuronal Interact. 2016 Sep 7;16(3):247-55. J Musculoskelet Neuronal Interact. 2016. PMID: 27609039 Free PMC article.
-
A growth area: A review of the value of clinical studies of child growth for palaeopathology.Evol Med Public Health. 2022 Feb 8;10(1):108-122. doi: 10.1093/emph/eoac005. eCollection 2022. Evol Med Public Health. 2022. PMID: 35273803 Free PMC article. Review.
-
Associations between serum levels of insulin-like growth factor-I and bone mineral acquisition in pubertal children: a 3-year follow-up study in Hamamatsu, Japan.J Physiol Anthropol. 2019 Dec 5;38(1):16. doi: 10.1186/s40101-019-0210-5. J Physiol Anthropol. 2019. PMID: 31806017 Free PMC article.
-
Age- and Sex-Related Volumetric Density Differences in Trabecular and Cortical Bone of the Proximal Femur in Healthy Population.J Bone Metab. 2024 Nov;31(4):279-289. doi: 10.11005/jbm.24.765. Epub 2024 Nov 30. J Bone Metab. 2024. PMID: 39701108 Free PMC article.
References
-
- Cooper C, Westlake S, Harvey N, Javaid K, Dennison E, et al. (2006) Review: developmental origins of osteoporotic fractures. Osteoporos Int 17: 337–347. - PubMed
-
- Rauch F, Glorieux FH (2004) Osteogenesis imperfecta. Lancet 363: 1377–1385. - PubMed
-
- Henderson RC, Lark RK, Gurka MJ, Worley G, Fung EB, et al. (2002) Bone density and metabolism in children and adolescents with moderate to severe cerebral palsy. Pediatrics 110(1Pt1): e5. - PubMed
-
- Soliman AT, Banna NE, Fattah MA, Eizalabani MM, Ansari BM (1998) Bone mineral density in prepubertal children with β-thalassemia: correlation with growth and hormonal data. Metabolism 47: 541–548. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
