

Risk of myocardial infarction and stroke in bipolar disorder: a systematic review and exploratory meta-analysis
- PMID: 24850482
- PMCID: PMC5023016
- DOI: 10.1111/acps.12293
Risk of myocardial infarction and stroke in bipolar disorder: a systematic review and exploratory meta-analysis
Abstract
Objective: To review the evidence on and estimate the risk of myocardial infarction and stroke in bipolar disorder.
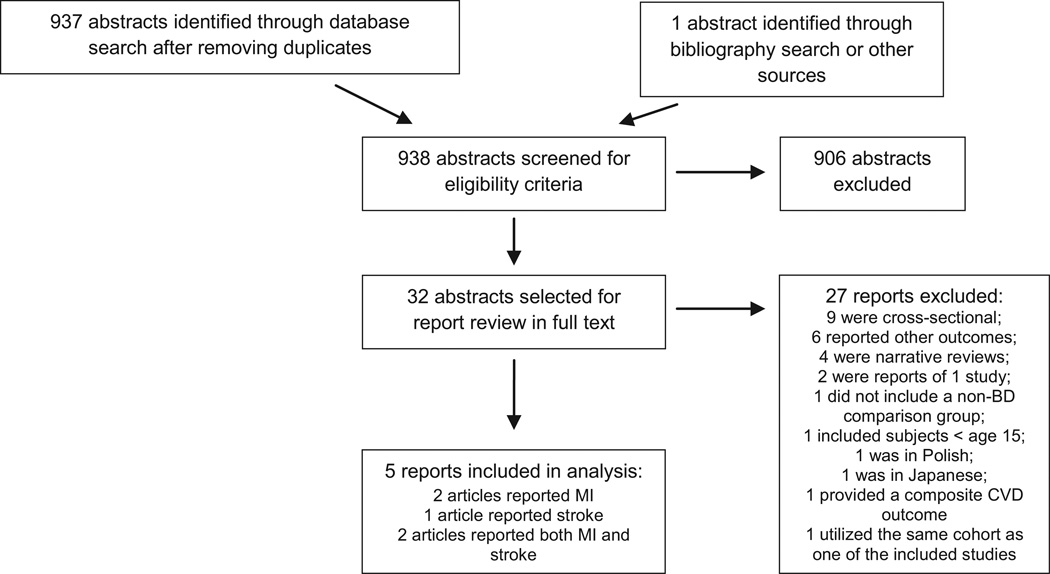
Method: A systematic search using MEDLINE, EMBASE, PsycINFO, Web of Science, Scopus, Cochrane Database of Systematic Reviews, and bibliographies (1946 - May, 2013) was conducted. Case-control and cohort studies of bipolar disorder patients age 15 or older with myocardial infarction or stroke as outcomes were included. Two independent reviewers extracted data and assessed quality. Estimates of effect were summarized using random-effects meta-analysis.
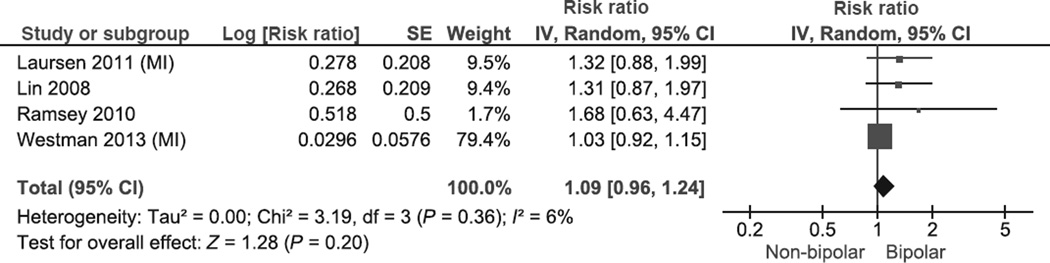
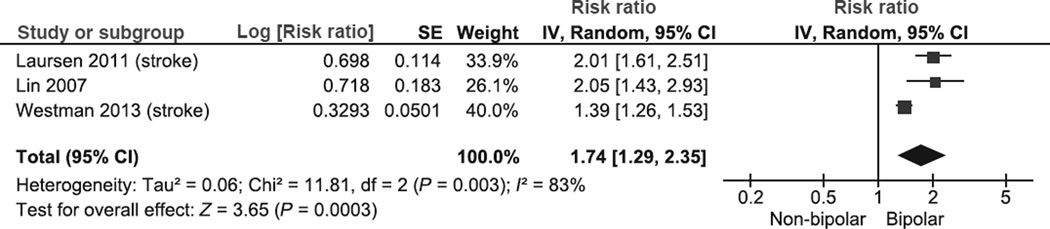
Results: Five cohort studies including 13 115 911 participants (27 092 bipolar) were included. Due to the use of registers, different statistical methods, and inconsistent adjustment for confounders, there was significant methodological heterogeneity among studies. The exploratory meta-analysis yielded no evidence for a significant increase in the risk of myocardial infarction: [relative risk (RR): 1.09, 95% CI 0.96-1.24, P = 0.20; I(2) = 6%]. While there was evidence of significant study heterogeneity, the risk of stroke in bipolar disorder was significantly increased (RR 1.74, 95% CI 1.29-2.35; P = 0.0003; I(2) = 83%).
Conclusion: There may be a differential risk of myocardial infarction and stroke in patients with bipolar disorder. Confidence in these pooled estimates was limited by the small number of studies, significant heterogeneity and dissimilar methodological features.
Keywords: bipolar disorder; cardiovascular diseases; meta-analysis; myocardial infarction; stroke.
© 2014 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Conflict of interest statement
Declaration of interestThis project was partially supported by Grant Number UL1 TR000135 from the National Center for Advancing Translational Sciences (NCATS). Its contents are solely the responsibility of the authors and do not necessarily represent the official views of the NIH. It was also partially supported by Mayo Foundation for Medical Education and Research. Dr. Prieto has received honoraria for speaker activities and development of educational presentations from GlaxoSmithKline, has received travel support from GlaxoSmithKline, Lilly, Lundbeck, Pharmavita, and has received scholarship support from the Government of Chile. Dr. Bellivier has received honoraria for speaker activities from AstraZeneca, Bristol-Myers Squibb, Euthérapie, Lundbeck, Otsuka, European Space Agency, and for consulting from Bristol-Myers Squibb, Lundbeck, Otsuka, European Space Agency. Dr. Frye has been a consultant (unpaid) for Allergan, Merck, Myriad, Sanofi-Aventis, Sunovion, Takeda Global Research, Teva Pharmaceuticals, United Biosource Corporation, has received grant support from Myriad, Pfizer, National Alliance for Schizophrenia and Depression (NARSAD), National Institute of Mental Health (NIMH), National Institute of Alcohol Abuse and Alcoholism (NIAAA), Mayo Foundation, and has received travel support from Chilean Society of Neurology, Psychiatry and Neurosurgery (Sociedad de Neurologia, Psiquiatria y Neurocirugia), Advanced Health Media, GlaxoSmithKline, Colombian Society of Neuropsychopharmacology, AstraZeneca, Bristol-Myers-Squib, Otsuka, Sanofi-Aventis. For the remaining authors, no further conflict of interests were declared.
Figures
References
-
- Frye MA. Clinical practice. Bipolar disorder–a focus on depression. N Engl J Med. 2011;364:51–59. - PubMed
-
- Magalhaes PV, Kapczinski F, Nierenberg AA, et al. Illness burden and medical comorbidity in the Systematic Treatment Enhancement Program for Bipolar Disorder. Acta Psychiatr Scand. 2012;125:303–308. - PubMed
-
- Osby U, Brandt L, Correia N, Ekbom A, Sparen P. Excess mortality in bipolar and unipolar disorder in Sweden. Arch Gen Psychiatry. 2001;58:844–850. - PubMed
-
- Castagnini A, Foldager L, Bertelsen A. Excess mortality of acute and transient psychotic disorders: comparison with bipolar affective disorder and schizophrenia. Acta Psychiatr Scand. 2013;128:370–375. - PubMed
-
- Hansson GK. Inflammation, atherosclerosis, and coronary artery disease. N Engl J Med. 2005;352:1685–1695. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
