

MR myelography for identification of spinal CSF leak in spontaneous intracranial hypotension
- PMID: 24852289
- PMCID: PMC7966231
- DOI: 10.3174/ajnr.A3975
MR myelography for identification of spinal CSF leak in spontaneous intracranial hypotension
Abstract
Background and purpose: CT myelography has historically been the test of choice for localization of CSF fistula in patients with spontaneous intracranial hypotension. This study evaluates the additional benefits of intrathecal gadolinium MR myelography in the detection of CSF leak.
Materials and methods: We performed a retrospective review of patients with spontaneous intracranial hypotension who underwent CT myelography followed by intrathecal gadolinium MR myelography. All patients received intrathecal iodine and off-label gadolinium-based contrast followed by immediate CT myelography and subsequent intrathecal gadolinium MR myelography with multiplanar T1 fat-suppressed sequences. CT myelography and intrathecal gadolinium MR myelography images were reviewed by an experienced neuroradiologist to determine the presence of CSF leak. Patient records were reviewed for demographic data and adverse events following the procedure.
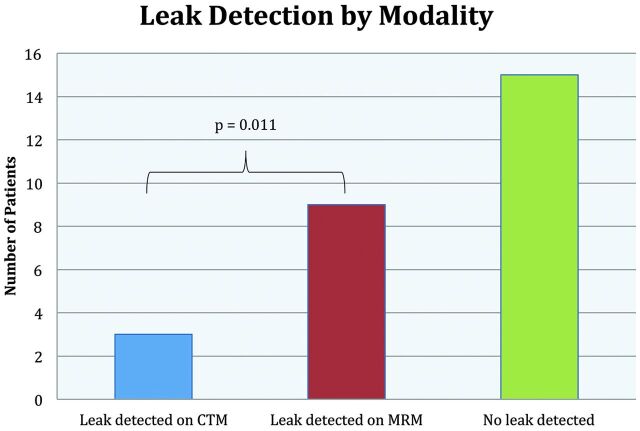
Results: Twenty-four patients met both imaging and clinical criteria for spontaneous intracranial hypotension and underwent CT myelography followed by intrathecal gadolinium MR myelography. In 3/24 patients (13%), a CSF leak was demonstrated on both CT myelography and intrathecal gadolinium MR myelography, and in 9/24 patients (38%), a CSF leak was seen on intrathecal gadolinium MR myelography (P = .011). Four of 6 leaks identified independently by intrathecal gadolinium MR myelography related to meningeal diverticula. CT myelography did not identify any leaks independently. There were no reported adverse events.
Conclusions: Present data demonstrate a higher rate of leak detection with intrathecal gadolinium MR myelography when investigating CSF leaks in our cohort of patients with spontaneous intracranial hypotension. Although intrathecal gadolinium is an FDA off-label use, all patients tolerated the medication without evidence of complications. Our data suggest that intrathecal gadolinium MR myelography is a well-tolerated examination with significant benefit in the evaluation of CSF leak, particularly for patients with leak related to meningeal diverticula.
© 2014 by American Journal of Neuroradiology.
Figures

References
-
- Schievink WI. Misdiagnosis of spontaneous intracranial hypotension. Arch Neurol 2003;60:1713–18 - PubMed
-
- Schievink WI. Spontaneous spinal cerebrospinal fluid leaks and intracranial hypotension. JAMA 2006;295:2286–96 - PubMed
-
- Rapport RL, Hillier D, Scearce T, et al. Spontaneous intracranial hypotension from intradural thoracic disc herniation: case report. J Neurosurg 2003;98(3 suppl):282–84 - PubMed
-
- Mokri B. Spontaneous cerebrospinal fluid leaks: from intracranial hypotension to cerebrospinal fluid hypovolemia—evolution of a concept. Mayo Clin Proc 1999;74:1113–23 - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous