

Association between intraoperative electroencephalographic suppression and postoperative mortality
- PMID: 24852500
- PMCID: PMC4433498
- DOI: 10.1093/bja/aeu105
Association between intraoperative electroencephalographic suppression and postoperative mortality
Abstract
Background: Low bispectral index values frequently reflect EEG suppression and have been associated with postoperative mortality. This study investigated whether intraoperative EEG suppression was an independent predictor of 90 day postoperative mortality and explored risk factors for EEG suppression.
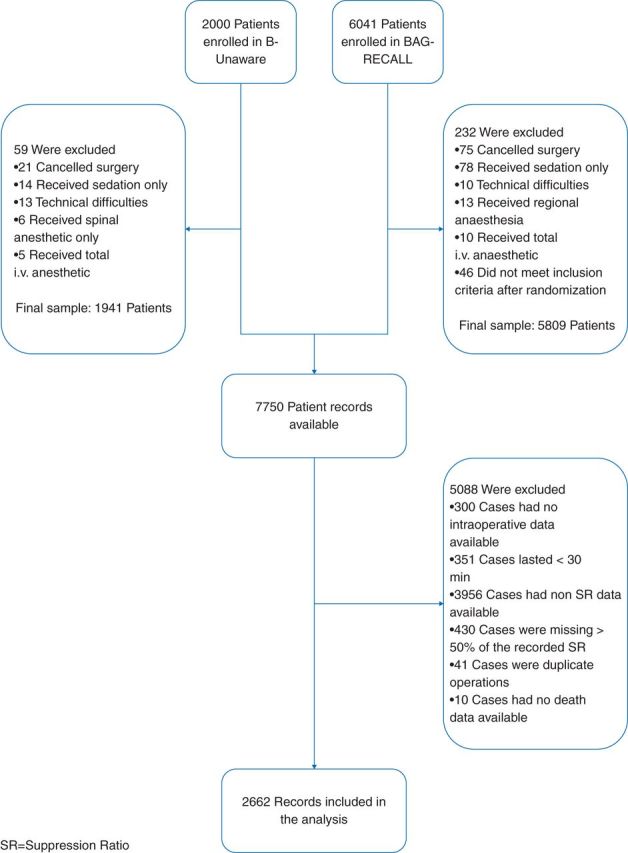
Methods: This observational study included 2662 adults enrolled in the B-Unaware or BAG-RECALL trials. A cohort was defined with >5 cumulative minutes of EEG suppression, and 1:2 propensity-matched to a non-suppressed cohort (≤5 min suppression). We evaluated the association between EEG suppression and mortality using multivariable logistic regression, and examined risk factors for EEG suppression using zero-inflated mixed effects analysis.
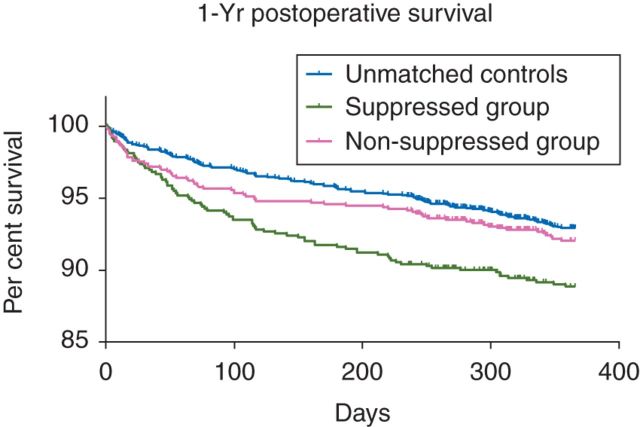
Results: Ninety day postoperative mortality was 3.9% overall, 6.3% in the suppressed cohort, and 3.0% in the non-suppressed cohort {odds ratio (OR) [95% confidence interval (CI)]=2.19 (1.48-3.26)}. After matching and multivariable adjustment, EEG suppression was not associated with mortality [OR (95% CI)=0.83 (0.55-1.25)]; however, the interaction between EEG suppression and mean arterial pressure (MAP) <55 mm Hg was [OR (95% CI)=2.96 (1.34-6.52)]. Risk factors for EEG suppression were older age, number of comorbidities, chronic obstructive pulmonary disease, and higher intraoperative doses of benzodiazepines, opioids, or volatile anaesthetics. EEG suppression was less likely in patients with cancer, preoperative alcohol, opioid or benzodiazepine consumption, and intraoperative nitrous oxide exposure.
Conclusions: Although EEG suppression was associated with increasing anaesthetic administration and comorbidities, the hypothesis that intraoperative EEG suppression is a predictor of postoperative mortality was only supported if it was coincident with low MAP.
Clinical trial registration: NCT00281489 and NCT00682825.
Keywords: anaesthesia, general; comorbidity; deep sedation; electroencephalography; risk assessment.
© The Author [2014]. Published by Oxford University Press on behalf of the British Journal of Anaesthesia. All rights reserved. For Permissions, please email: journals.permissions@oup.com.
Figures
Comment in
-
'Known unknowns and unknown unknowns': electroencephalographic burst suppression and mortality.Br J Anaesth. 2014 Dec;113(6):897-9. doi: 10.1093/bja/aeu147. Epub 2014 May 29. Br J Anaesth. 2014. PMID: 24875662 No abstract available.
-
Does anaesthetic dose really not contribute to mortality?Br J Anaesth. 2015 Oct;115(4):638. doi: 10.1093/bja/aev315. Br J Anaesth. 2015. PMID: 26385677 No abstract available.
References
-
- Noordzij PG, Poldermans D, Schouten O, Bax JJ, Schreiner FAG, Boersma E. Postoperative mortality in the Netherlands. Anesthesiology. 2010;112:1105–15. - PubMed
-
- Kertai MD, Pal N, Palanca BJ, et al. Association of perioperative risk factors and cumulative duration of low bispectral index with intermediate-term mortality after cardiac surgery in the B-Unaware Trial. Anesthesiology. 2010;112:1116–27. - PubMed
-
- Damhuis RAM, Wijnhoven BPL, Plaisier PW, Kirkels WJ, Kranse R, van Lanschot JJ. Comparison of 30-day, 90-day and in-hospital postoperative mortality for eight different cancer types. Br J Surg. 2012;99:1149–54. - PubMed
-
- Monk TG, Saini V, Weldon BC, Sigl JC. Anesthetic management and one-year mortality after noncardiac surgery. Anesth Analg. 2005;100:4–10. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
