

Increased fluid administration in the first three hours of sepsis resuscitation is associated with reduced mortality: a retrospective cohort study
- PMID: 24853382
- PMCID: PMC4188147
- DOI: 10.1378/chest.13-2702
Increased fluid administration in the first three hours of sepsis resuscitation is associated with reduced mortality: a retrospective cohort study
Abstract
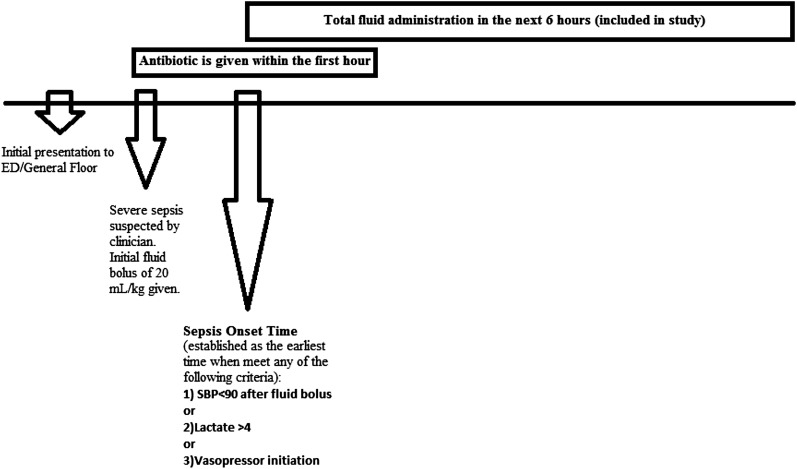
Background: The surviving sepsis guidelines recommend early aggressive fluid resuscitation within 6 h of sepsis onset. Although rapid fluid administration may offer benefit, studies on the timing of resuscitation are lacking. We hypothesized that there is an association between quicker, adequate fluid resuscitation and patient outcome from sepsis onset time.
Methods: This is a retrospective cohort study of consecutive adults with severe sepsis and septic shock admitted to a quaternary care medical ICU between January 2007 and December 2009. Data were collected from a previously validated electronic medical database. Multivariate regression modeling was performed, adjusting for age, admission weight, Sequential Organ Failure Assessment score, APACHE (Acute Physiology and Chronic Health Examination) III score, and total fluid administration within the first 6 h of sepsis onset time.
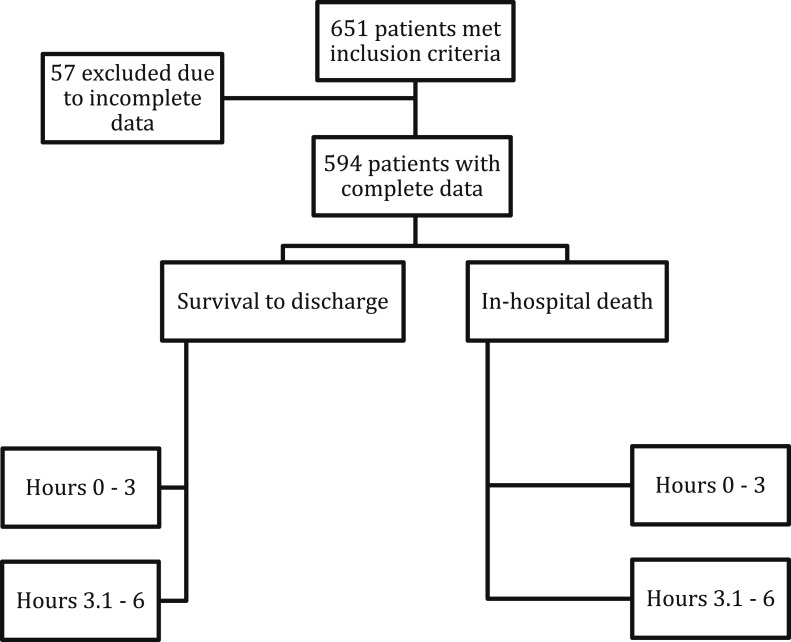
Results: Of 651 patients with severe sepsis and septic shock screened, 594 had detailed fluid data. In a univariate analysis, the median amount of fluid within the first 3 h for survivors at discharge was 2,085 mL (940-4,080 mL) and for nonsurvivors, 1,600 mL (600-3,010 mL; P = .007). In comparison, during the latter 3 h, the median amount was 660 mL (290-1,485 mL) vs 800 mL (360-1,680 mL; P = .09), respectively. After adjusting for confounders, the higher proportion of total fluid received within the first 3 h was associated with decreased hospital mortality (OR, 0.34; 95% CI, 0.15-0.75; P = .008).
Conclusions: Earlier fluid resuscitation (within the first 3 h) is associated with a greater number of survivors with severe sepsis and septic shock.
Figures
Comment in
-
Higher fluids in the first three hours of sepsis resuscitation? Too soon to conclude.Chest. 2014 Nov;146(5):e180. doi: 10.1378/chest.14-1256. Chest. 2014. PMID: 25367496 No abstract available.
-
Response.Chest. 2014 Nov;146(5):e181. doi: 10.1378/chest.14-1712. Chest. 2014. PMID: 25367497 No abstract available.
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29(7):1303-1310 - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348(16):1546-1554 - PubMed
-
- Kaukonen KM, Bailey M, Suzuki S, Pilcher D, Bellomo R. Mortality related to severe sepsis and septic shock among critically ill patients in Australia and New Zealand, 2000-2012. JAMA. 2014;311(13):1308-1316 - PubMed
-
- Hall MJ, Williams SN, DeFrances CJ, Golosinskiy A. Inpatient care for septicemia or sepsis: a challenge for patients and hospitals. NCHS Data Brief. 2011;(62): 1-8 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
