

Nephrotic syndrome: components, connections, and angiopoietin-like 4-related therapeutics
- PMID: 24854282
- PMCID: PMC4214538
- DOI: 10.1681/ASN.2014030267
Nephrotic syndrome: components, connections, and angiopoietin-like 4-related therapeutics
Abstract
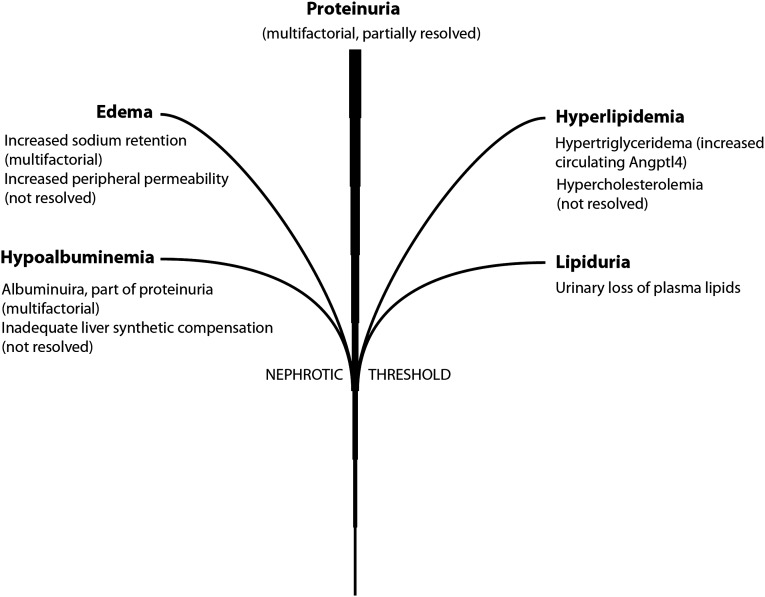
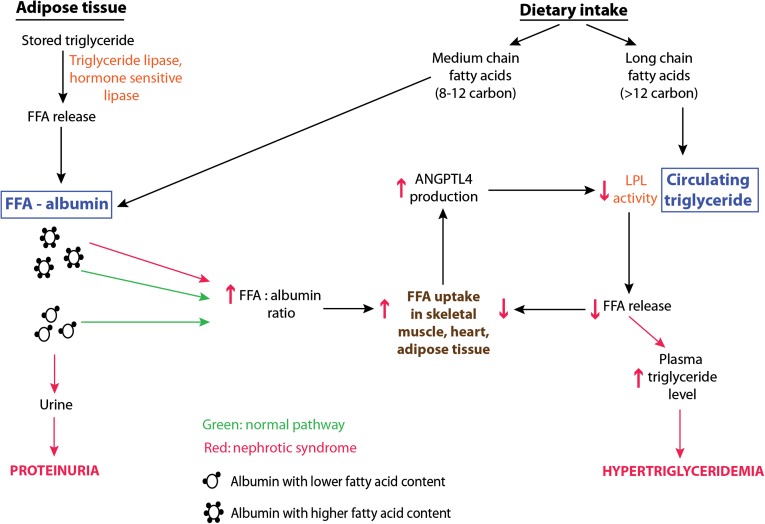
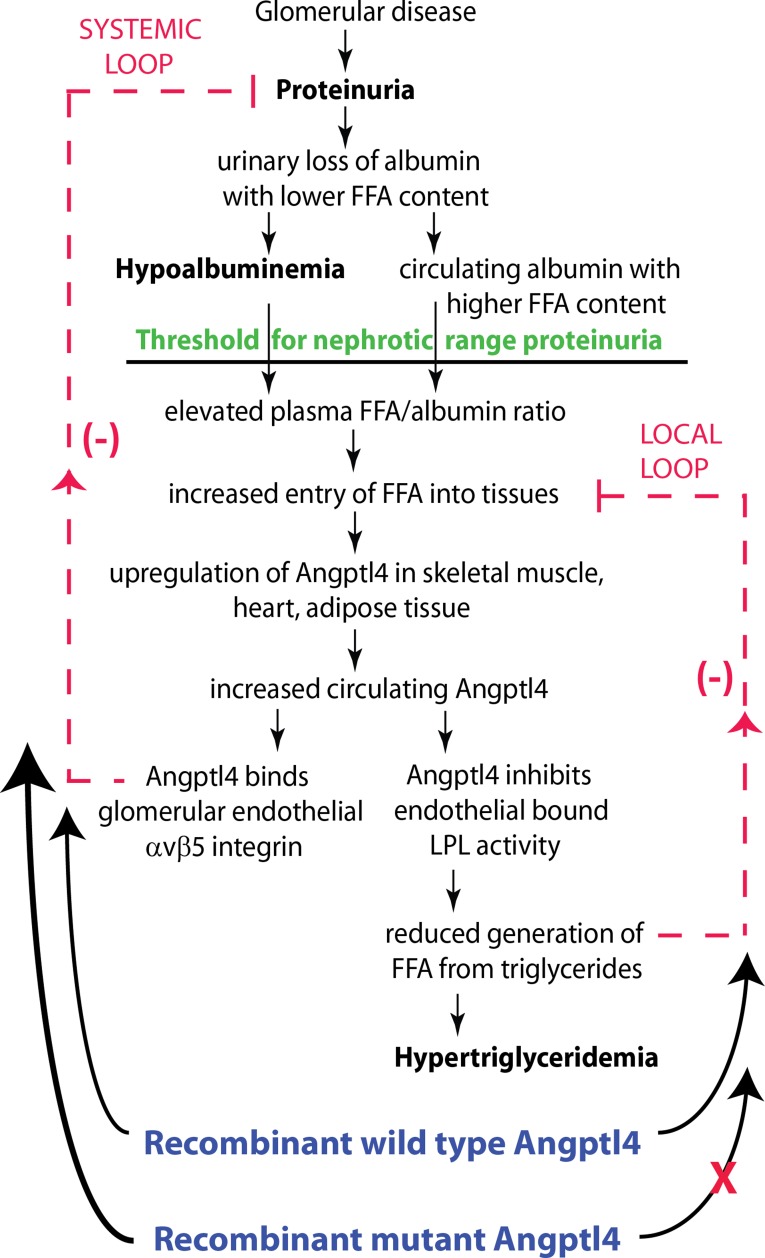
Nephrotic syndrome is recognized by the presence of proteinuria in excess of 3.5 g/24 h along with hypoalbuminemia, edema, hyperlipidemia (hypertriglyceridemia and hypercholesterolemia), and lipiduria. Each component has been investigated individually over the past four decades with some success. Studies published recently have started unraveling the molecular basis of proteinuria and its relationship with other components. We now have improved understanding of the threshold for nephrotic-range proteinuria and the pathogenesis of hypertriglyceridemia. These studies reveal that modifying sialylation of the soluble glycoprotein angiopoietin-like 4 or changing key amino acids in its sequence can be used successfully to treat proteinuria. Treatment strategies on the basis of fundamental relationships among different components of nephrotic syndrome use naturally occurring pathways and have great potential for future development into clinically relevant therapeutic agents.
Keywords: FSGS; diabetic nephropathy; lipids; nephrotic syndrome; podocyte; proteinuria.
Copyright © 2014 by the American Society of Nephrology.
Figures
References
-
- Clement LC, Liu G, Perez-Torres I, Kanwar YS, Avila-Casado C, Chugh SS: Early changes in gene expression that influence the course of primary glomerular disease. Kidney Int 72: 337–347, 2007 - PubMed
-
- Kestilä M, Lenkkeri U, Männikkö M, Lamerdin J, McCready P, Putaala H, Ruotsalainen V, Morita T, Nissinen M, Herva R, Kashtan CE, Peltonen L, Holmberg C, Olsen A, Tryggvason K: Positionally cloned gene for a novel glomerular protein—nephrin—is mutated in congenital nephrotic syndrome. Mol Cell 1: 575–582, 1998 - PubMed
-
- Boute N, Gribouval O, Roselli S, Benessy F, Lee H, Fuchshuber A, Dahan K, Gubler MC, Niaudet P, Antignac C: NPHS2, encoding the glomerular protein podocin, is mutated in autosomal recessive steroid-resistant nephrotic syndrome. Nat Genet 24: 349–354, 2000 - PubMed
-
- Donoviel DB, Freed DD, Vogel H, Potter DG, Hawkins E, Barrish JP, Mathur BN, Turner CA, Geske R, Montgomery CA, Starbuck M, Brandt M, Gupta A, Ramirez-Solis R, Zambrowicz BP, Powell DR: Proteinuria and perinatal lethality in mice lacking NEPH1, a novel protein with homology to NEPHRIN. Mol Cell Biol 21: 4829–4836, 2001 - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
