

A composite index for predicting readmission following emergency general surgery
- PMID: 24854317
- PMCID: PMC4806856
- DOI: 10.1097/TA.0000000000000223
A composite index for predicting readmission following emergency general surgery
Abstract
Background: Preventable readmission has become a national focus. It is clear that surgical patients present specific challenges to those interested in preventing readmission. Little is known about this outcome in the emergent population. We are interested in determining if there are readily available data variables to predict risk of readmission. The surgical Apgar score (SAS) is calculated from objective intraoperative variables and has been shown to be predictive of postoperative mortality in the nonemergent setting. The objectives of this study were to characterize 30-day readmissions in emergent general surgery and to determine whether certain variables were associated with readmissions. We hypothesized that the SAS correlates with the risk for readmission in emergency general surgery patients.
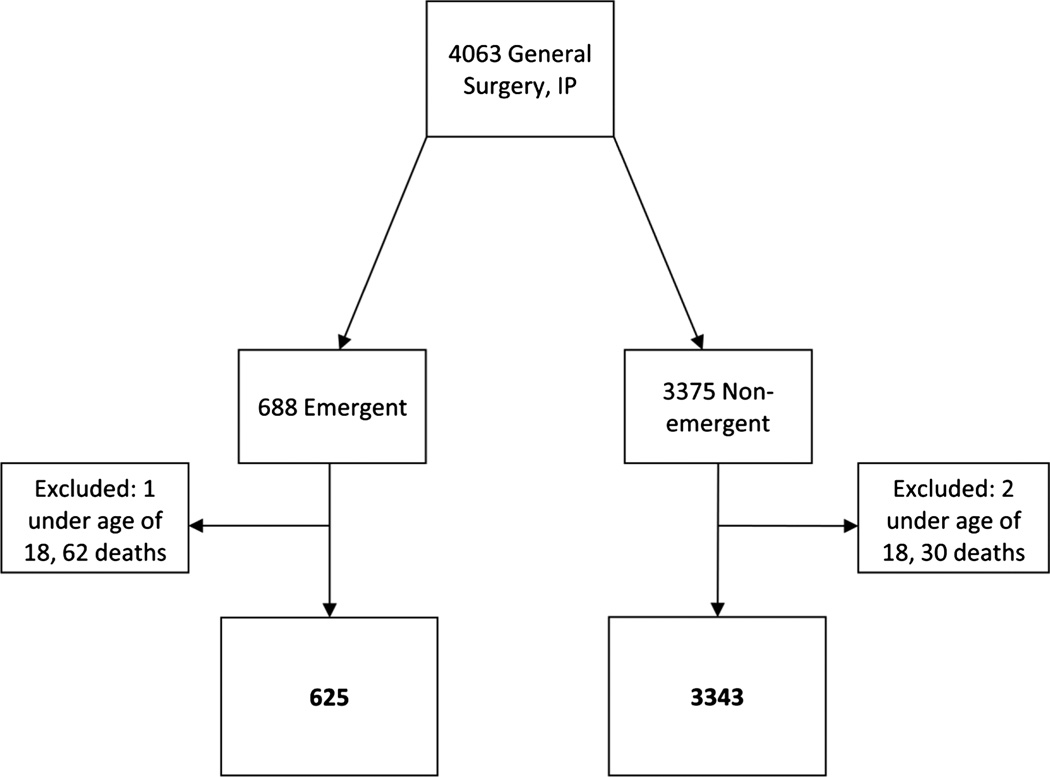
Patients and methods: Variables of interest were obtained from a retrospective analysis of the American College of Surgeons' National Surgical Quality Improvement Program database at an academic institution, paired with the electronic medical record. We identified adult general surgery patients who underwent an emergency procedure from 2006 to 2012. Univariate analysis identified factors associated with 30-day readmission. Factors with p < 0.1 were included in the multivariate analysis to reveal potential risk factors. SPSS version 20 was used for the statistical analysis, with p < 0.05 considered to be significant on multivariate analysis.
Results: As compared with nonemergency surgery patients, emergency surgery patients had a higher readmission rate (11.1% vs. 15.2%, p = 0.004). The SAS (odds ratio, 3.297; 95% confidence interval, 1.074-10.121; p = 0.037) and the combined variable of the American Society of Anesthesiologists Physical Status Classification and length of stay (odds ratio, 4.370; 95% confidence interval, 2.251-8.486; p < 0.001) were associated with elevated risk for readmission in emergency general surgery patients.
Conclusion: We have identified readily available measures that allow for the stratification of patients into low- and high-risk groups for 30-day readmission. The stratification of patients will enable the study of prospective interventions designed to decrease unplanned readmissions in emergency surgery patients.
Level of evidence: Prognostic study, level II.
Figures
References
-
- Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360:1418–1428. - PubMed
-
- Lawson EH, Hall BL, Louie R, Ettner SL, Zingmond DS, Han L, Rapp M, Ko CY. Association Between Occurrence of a Postoperative Complication and Readmission: Implications for Quality Improvement and Cost Savings. Annals of Surgery. 2013;258:10–18. - PubMed
-
- Reynolds PQ, Sanders NW, Schildcrout JS, Mercaldo ND, St Jacques PJ. Expansion of the surgical Apgar score across all surgical subspecialties as a means to predict postoperative mortality. Anesthesiology. 2011;114:1305–1312. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
