

Maternal factors and complications of preterm birth associated with neonatal thyroid stimulating hormone
- PMID: 24854527
- PMCID: PMC4260397
- DOI: 10.1515/jpem-2013-0366
Maternal factors and complications of preterm birth associated with neonatal thyroid stimulating hormone
Abstract
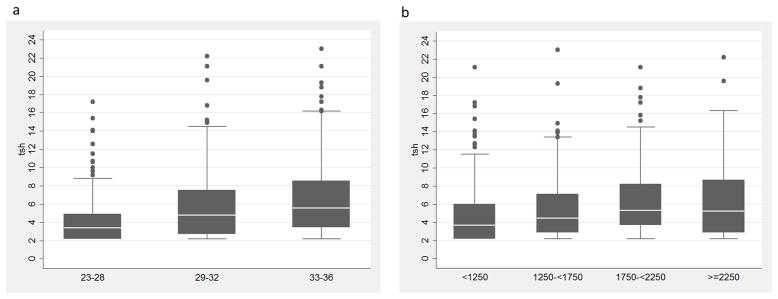
Thyroid hormones are important regulators of fetal neurodevelopment. Among preterm infants, thyroid stimulating hormone (TSH) is highly variable. Understanding this variability will further improvements in screening for thyroid disorders in preterm infants. We examined 61 maternal and infant clinical and demographic factors for associations with neonatal TSH levels in 698 preterm neonates. TSH was measured as part of routine State-mandated newborn screening in Iowa. Of the maternal characteristics, nulliparous women (p=8×10-4), women with preeclampsia (p=2×10-3), and those with induced labor (p=3×10-3) had infants with higher TSH levels. TSH levels at the time of newborn screening were associated with respiratory distress syndrome (RDS) (p<0.0001) and sepsis (p=3×10-3). We replicated findings between parity and preeclampsia previously observed in primarily term infants. We also observed strong relationships between neonatal TSH and complications of prematurity including RDS and sepsis, which have implications for future studies examining this relationship both prenatally and longitudinally after birth.
Conflict of interest statement
No competing financial interests exist.
Figures
References
-
- Medici M, de Rijke YB, Peeters RP, Visser W, de Muinck Keizer-Schrama SM, Jaddoe VV, Hofman A, Hooijkaas H, Steegers EA, Tiemeier H, Bongers-Schokking JJ, Visser TJ. Maternal early pregnancy and newborn thyroid hormone parameters: The generation R study. J Clin Endocrinol Metab. 2012;97(2):646–52. - PubMed
-
- Wilson KL, Casey BM, McIntire DD, Halvorson LM, Cunningham FG. Subclinical thyroid disease and the incidence of hypertension in pregnancy. Obstet Gynecol. 2012;119(2 Pt 1):315–20. - PubMed
-
- Schneuer FJ, Nassar N, Tasevski V, Morris JM, Roberts CL. Association and predictive accuracy of high TSH serum levels in first trimester and adverse pregnancy outcomes. J Clin Endocrinol Metab. 2012;97(9):3115–22. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources