

Gut microbiome and colorectal adenomas
- PMID: 24855012
- PMCID: PMC4589167
- DOI: 10.1097/PPO.0000000000000050
Gut microbiome and colorectal adenomas
Abstract
The trillions of bacteria that naturally reside in the human gut collectively constitute the complex system known the gut microbiome, a vital player for the host's homeostasis and health. However, there is mounting evidence that dysbiosis, a state of pathological imbalance in the gut microbiome is present in many disease states. In this review, we present recent insights concerning the gut microbiome's contribution to the development of colorectal adenomas and the subsequent progression to colorectal cancer (CRC). In the United States alone, CRC is the second leading cause of cancer deaths. As a result, there is a high interest in identifying risk factors for adenomas, which are intermediate precursors to CRC. Recent research on CRC and the microbiome suggest that modulation of the gut bacterial composition and structure may be useful in preventing adenomas and CRC. We highlight the known risk factors for colorectal adenomas and the potential mechanisms by which microbial dysbiosis may contribute to the etiology of CRC. We also underscore novel findings from recent studies on the gut microbiota and colorectal adenomas along with current knowledge gaps. Understanding the microbiome may provide promising new directions towards novel diagnostic tools, biomarkers, and therapeutic interventions for CRC.
Figures

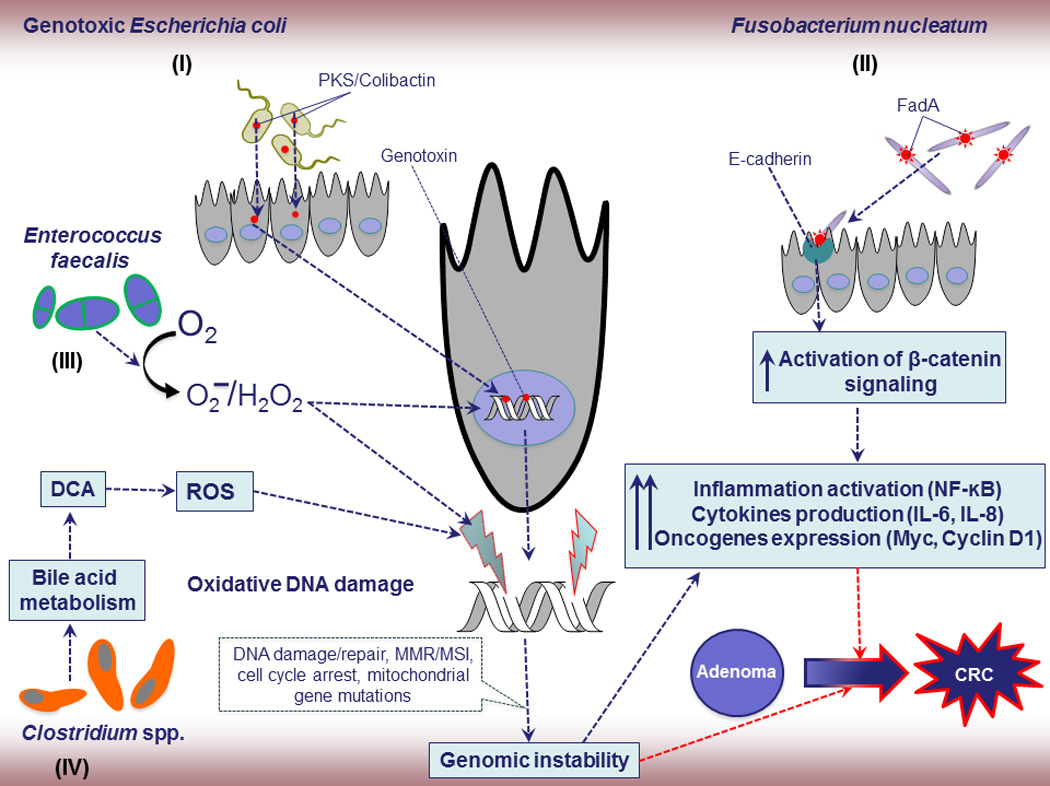
E. coli, Gram-negative facultative anaerobic bacterium, considered as one of the potential etiological agents of CRC due to its genotoxins such as Colibactin, and cytolethal distending toxin (CDT). These products could induce DNA damage and influence the progression of CRC due to genomic instability from MSI, MMR, and mutations.
F. nucleatum, Gram-negative anaerobic bacterium, has been linked to CRC progression but the exact underlying mechanisms are still unknown. A potential F. nucleatum-driven CRC mechanism is its invasion into epithelial cells and activation of oncogenic and inflammatory responses through its unique FadA adhesin. Active FadA binds to E-cadherin, mediating Fusobacterium attachment and invasion into the epithelial cells. This activates β-catenin signaling, leading to increased activation of inflammatory genes (NF-κB) and secretion of cytokines interleukin-6 (IL-6), IL-8, and IL-18, and oncogenes and drives to adenoma to adenocarcinoma.
E. faecalis, has been shown to produce extracellular superoxide and hydrogen peroxide, which damage DNA and also further enhances chromosomal instability in colonic epithelial cells. Chromosomal instability, a common cause of genomic instability in tumors, is characterized by nucleotide additions or deletions, inversions, translocations, and complex rearrangements, and ultimately contributes to the dramatic and unstable alteration in genomic state critical for tumor initiation in the colorectum.
Gram-positive, spore forming bacteria in cluster IX of the genus Clostridium spp. convert primary bile acids into a secondary bile acid such as deoxycholic acid (DCA). DCA is widely considered as a carcinogen that is associated with DNA damage via the production of free radicals or reactive oxygen species (ROS) and implicated to adenoma-inflammation-CRC through enhancing genomic instability and inflammation.
E. coli, Gram-negative facultative anaerobic bacterium, considered as one of the potential etiological agents of CRC due to its genotoxins such as Colibactin, and cytolethal distending toxin (CDT). These products could induce DNA damage and influence the progression of CRC due to genomic instability from MSI, MMR, and mutations.
F. nucleatum, Gram-negative anaerobic bacterium, has been linked to CRC progression but the exact underlying mechanisms are still unknown. A potential F. nucleatum-driven CRC mechanism is its invasion into epithelial cells and activation of oncogenic and inflammatory responses through its unique FadA adhesin. Active FadA binds to E-cadherin, mediating Fusobacterium attachment and invasion into the epithelial cells. This activates β-catenin signaling, leading to increased activation of inflammatory genes (NF-κB) and secretion of cytokines interleukin-6 (IL-6), IL-8, and IL-18, and oncogenes and drives to adenoma to adenocarcinoma.
E. faecalis, has been shown to produce extracellular superoxide and hydrogen peroxide, which damage DNA and also further enhances chromosomal instability in colonic epithelial cells. Chromosomal instability, a common cause of genomic instability in tumors, is characterized by nucleotide additions or deletions, inversions, translocations, and complex rearrangements, and ultimately contributes to the dramatic and unstable alteration in genomic state critical for tumor initiation in the colorectum.
Gram-positive, spore forming bacteria in cluster IX of the genus Clostridium spp. convert primary bile acids into a secondary bile acid such as deoxycholic acid (DCA). DCA is widely considered as a carcinogen that is associated with DNA damage via the production of free radicals or reactive oxygen species (ROS) and implicated to adenoma-inflammation-CRC through enhancing genomic instability and inflammation.
References
-
- GLOBOCON. IARC, WHO; 2012. Estimated cancer incidence, mortality and prevalence in 2012.
-
- Siegel R, Ma J, Zou Z, et al. Cancer statistics, 2014. CA: a cancer journal for clinicians. 2014;64:9–29. - PubMed
-
- Muto T, Bussey HJ, Morson BC. The evolution of cancer of the colon and rectum. Cancer. 1975;36:2251–2270. - PubMed
-
- Parente F, Bargiggia S, Boemo C, et al. Anatomic distribution of cancers and colorectal adenomas according to age and sex and relationship between proximal and distal neoplasms in an i-FOBT-positive average-risk Italian screening cohort. International journal of colorectal disease. 2014;29:57–64. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
